|
#1
●
10-09-2023, 03:50 PM
| ||||||||
| ♚ Legacy Gold Member ♚ Poster Rank:908 Join Date: Jul 2020 Posts: 820
Contributions: 10
Mentioned: 13 Post(s) Quoted: 173 Post(s)
| ||||||||
|
The Shocker's Mix 80
Some of the stuff I work on doesn't make the cut so I thought about gathering them up in a single post. So basically it's images I have little or no info about or I've decided that they don't get their own thread, for example, because of low image/content quality, lack of backstory or additional info/knowledge, possibly uninteresting, only one image but not very special. I still do the usual image work including upscaling and color correction as needed, as I prefer to have my content high quality and educational. - - - Case 1  Fig1.1 Multiple homicidal lacerations of the scalp. Multiple homicidal lacerations of the scalp. The unusual shape is difficult to interpret, but they were caused by a claw hammer. Two are triangular, the upper and lower show tissue bridges because of the gap between the two claws. - - - Case 2  Fig2.1 Laceration of the scalp from a heavy torch. Laceration of the scalp from a 30 cm long heavy torch (insert). The skin over the shoulders is reddish due to first-and second-degree burns. The victim was hit on the head while sleeping in bed, after which the husband poured petrol over the body and set it on fire. - - - Case 3  Fig3.1 Homicidal lacerations of the scalp penetrating the skull. Homicidal lacerations of the scalp penetrating the skull. Although some of the injuries resemble incised wounds, their margins are crushed, and hairs and tissue strands cross the injuries. The damage was probably inflicted with a metal rod with sharp edges. - - - Case 4  Fig4.1 Mental patient commits suicide with a frame saw. 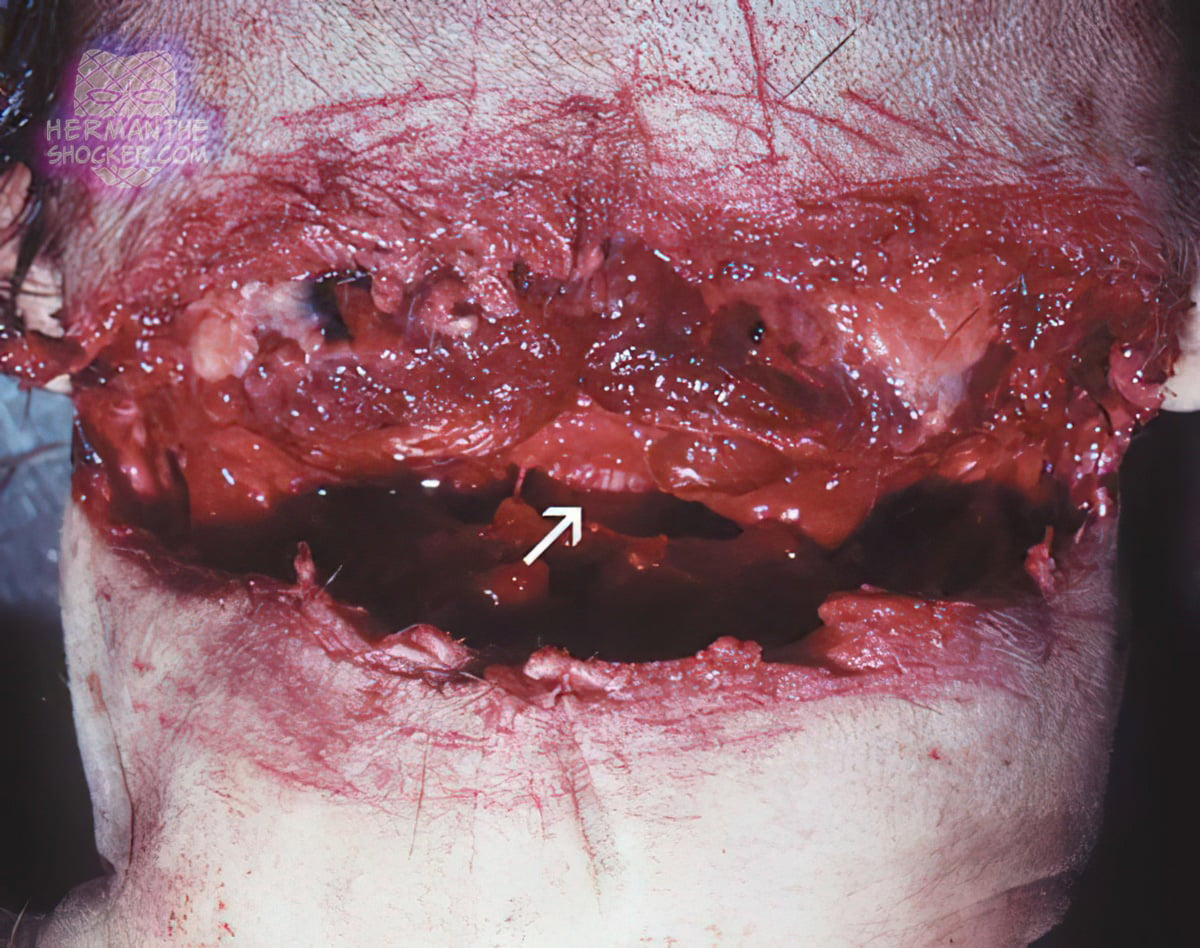 Fig4.2 Back of neck showing marks of the saw teeth around the laceration and medulla at the bottom (arrow). Gaping laceration in front of neck of a mental patient, who on leave from a psychiatric hospital, had used a frame saw to commit suicide. Arrow shows the marks of the saw teeth around the laceration and medulla at the bottom - - - Case 5 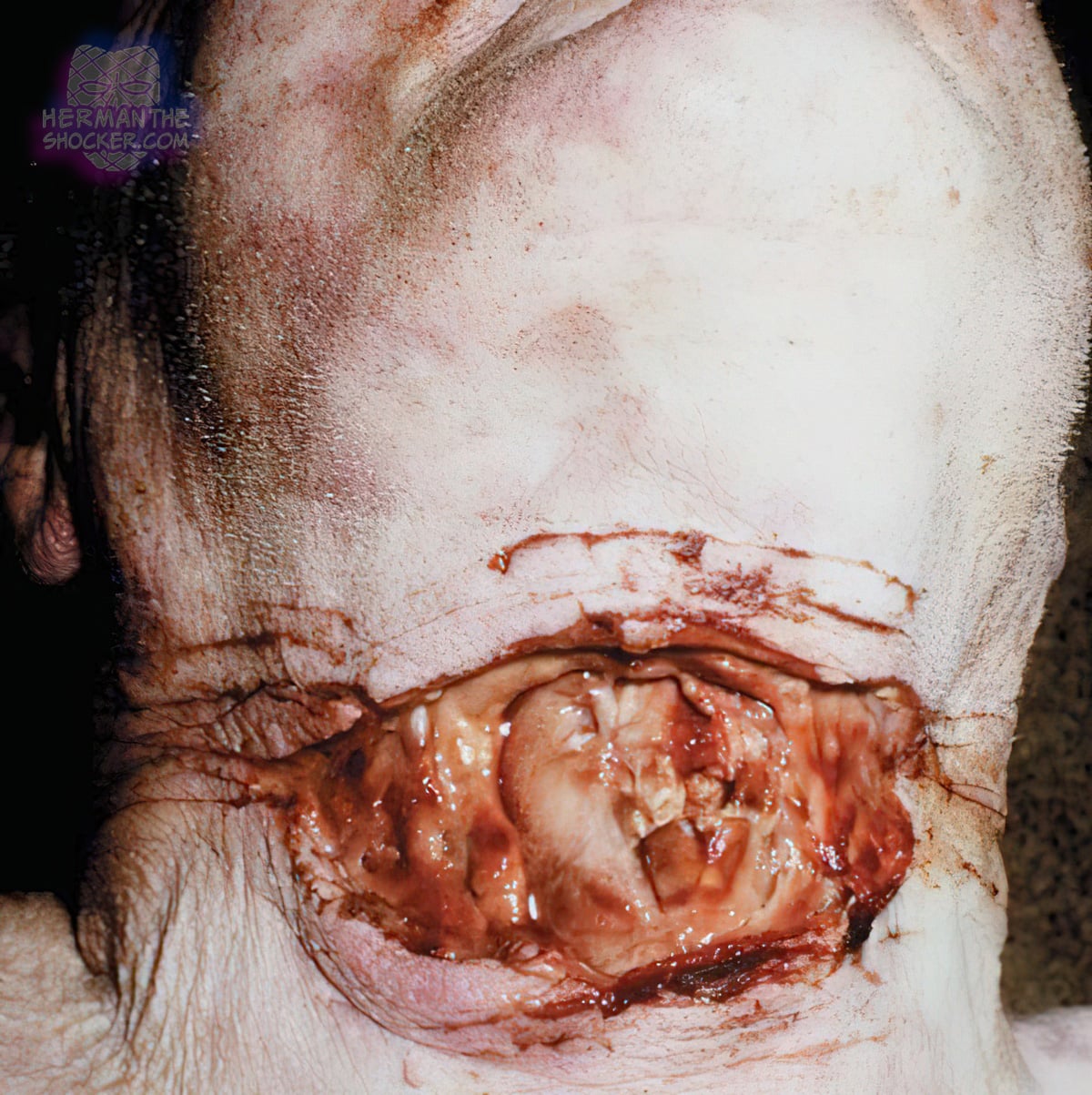 Fig5.1 Suicidal cut throat. Suicidal cut throat. The wounds are horizontal, rather than the more common sloping-down from left to right in a right- handed person. The numerous ‘tentative cuts’ are the hallmark of self-infliction, though there are rare exceptions. The larynx has been entered and death was due to aspiration of blood into the air passages. The great vessels in the neck were undamaged. - - - Case 6  Fig6.1 Suicidal firearm wound from a twelve-bore shotgun. Suicidal firearm wound from a twelve-bore shotgun. The wound shows a muzzle impression with soot soiling, the double-barrelled shotgun having been pressed against the skin at discharge. - - - Case 7  Fig7.1 Reconstruction of devastating head injuries. Crushing head injuries are characterized by extensive soft tissue laceration, closed and open comminuted fractures of cranial and facial parts of the skull, often in conjunction with laceration of the brain or its partial or total prolapse. This type of injury usually does not allow direct visual identification of individuals, and above all, it constitutes an obstacle to a comprehensive evaluation of discrete traumatic changes of the skin and soft tissues. Typical examples of the mechanisms that often lead to large, mutilating, and devastating head injuries include: gunshot injuries, explosions, high-energy injuries on railways and roads, falls from height (head-first impacts), injuries caused by solid objects, burial under the soil, stones, machine, etc. Case 1 A 64-year-old man committed suicide in a forest stand using a repeating hunting rifle (model CZ 550; ammunition caliber 308 W, projectile SPCE-soft point cutting edge, 150 gr). As a result, a devastating head injury with a complete exenteration of both brain hemispheres occurred (called Krönlein shot). The autopsy could not clearly determine the appearance of the primary gunshot wound, and the entrance and exit wounds were not identified with certainty. After reconstructing the skull bone and adapting the soft tissue with sutures, it was possible to identify precisely the entrance wound in the right temporal region, including the muzzle imprint and the fouling, as well as the exit wound at the crossing of the left temporal and parietal regions. After the reconstruction, the secondary tears of the facial skin and soft tissue were also easily identifiable, even when found at a greater distance from the primary injury. Full case report here - Part 1 --- Part 2 --- Part 3 --- Part 4 --- Part 5 --- Part 6 --- Part 7 --- Part 8 --- Part 9 --- Part 10 --- Part 11 --- Part 12 --- Part 13 --- Part 14 --- Part 15 --- Part 16 --- Part 17 --- Part 18 --- Part 19 --- Part 20 --- Part 21 --- Part 22 --- Part 23 --- Part 24 --- Part 25 --- Part 26 --- Part 27 --- Part 28 --- Part 29 --- Part 30 --- Part 31 --- Part 32 --- Part 33 --- Part 34 --- Part 35 --- Part 36 --- Part 37 --- Part 38 --- Part 39 --- Part 40 --- Part 41 --- Part 42 --- Part 43 --- Part 44 --- Part 45 --- Part 46 --- Part 47 --- Part 48 --- Part 49 --- Part 50 --- Part 51 --- Part 52 --- Part 53 --- Part 54 --- Part 55 --- Part 56 --- Part 57 --- Part 58 --- Part 59 --- Part 60 --- Part 61 --- Part 62 --- Part 63 --- Part 64 --- Part 65 --- Part 66 --- Part 67 --- Part 68 --- Part 69 --- Part 70 --- Part 71 --- Part 72 --- Part 73 --- Part 74 --- Part 75 --- Part 76 --- Part 77 --- Part 78 --- Part 79 - This post is for educational purposes only and is nonprofit. Under Section 107 of the US Copyright Act of 1976; Allowance is made for "Fair Use" for purposes such as criticism, comment, news reporting, teaching, scholarship, and research. OP is not a medical expert. No copyright infringement intended. This post does not encourage or glorify violence/harassment. Images might have been upscaled and enhanced. Text might have been shortened and simplified/reorganized for online view.
__________________ ⭐️ hermantheshocker.com ⭐️ |
|
#2
●
10-09-2023, 06:40 PM
| ||||||||
| ✖ The Antique Christ ✖ Poster Rank:105 Gonzo Punk Join Date: Jan 2009 Posts: 15,488
Contributions: 58
Mentioned: 23 Post(s) Quoted: 2046 Post(s)
| ||||||||
|
Re: The Shocker's Mix 80
Case 7 did a pretty good job considering what they had to work with. |




























{kind=link}