|
#1
●
01-16-2023, 02:11 PM
| ||||||||
| ♚ Legacy Gold Member ♚ Poster Rank:908 Join Date: Jul 2020 Posts: 820
Contributions: 10
Mentioned: 13 Post(s) Quoted: 173 Post(s)
| ||||||||
|
The Shocker's Mix 49
Some of the stuff I work on doesn't make the cut so I thought about gathering them up in a single post. So basically it's images I have little or no info about or I've decided that they don't get their own thread, for example, because of low image/content quality, lack of backstory or additional info/knowledge, possibly uninteresting, only one image but not very special. I still do the usual image work including upscaling and color correction as needed, as I prefer to have my content high quality and educational. - - - Case 1  Fig1.1 Close-range shotgun entrance wound. Seen here is a close-range shotgun entrance wound as evidenced by the slight scalloping of the wound edges and the angular abrasion on the surround- ing skin caused by the shell case (wadding) petals. This combination of findings is most compatible with a distance of 3 feet. It should be noted that this is an estimate of the range of fire. In order to ascertain the distance one must test fire the weapon with the ammunition used. - - - Case 2  Fig2.1 Mechanical asphyxia. The orientation of the decedent with the tire of the motor vehicle apparently compressing the midsection and with the corresponding vascular changes (congestion versus petechiae) support a scenario in which there was hampered venous return to the heart. As this would lead to impaired respiration, this is considered a form of mechanical asphyxia. - - - Case 3  Fig3.1 Suicidal cuts using a box cutter. The finding illustrated is a group of sharp force injuries (incisions) that are self-inflicted, as evidenced by the anterior location of the incisions and the presence of hesitation marks on the antecubital fossa, forearm, and wrist. - - - Case 4  Fig4.1 Woman assaulted from behind with knife. The photograph demonstrates a classic sweeping incised wound created by an individual standing behind the decedent. It should be noted, however, that a similar wound may be created from an assailant in front of the decedent if the knife is held differently. So, such conclusions are best left to the investigative team. - - - Case 5  Fig5.1 Stellate gunshot wound. Contact (entrance) gunshot wounds to the head often show large stellate defects, due to the explosive blast of the gases driven under the skin, with powder/soot blackening in the base of the wound. contact gunshot wounds are of great significance in the forensic setting, most often implying intentional self- inflicted injury, although close physical struggle and execution-style shootings must also be considered. these wounds always require accurate decsription, and close attention to the size, shape and appearance of the base and periphery of the wound. - - - Case 6  Fig6.1 Gunshot wound tattooing. Tattooing results fom close range discharge, with gunpowder particles being impregnated into the skin. The dispersion pattern and width may greatly assist in assessing the direction and/or distance of fire. handgun injuries from an intermediate range (usually between approximately 10 and 50 cm, where some powder may still be deposited on the target/victim) often require particularly close scrutiny, since tattooing may be difficult to see, especially in hairy parts of the body or in those with dark skin. - - - Case 7 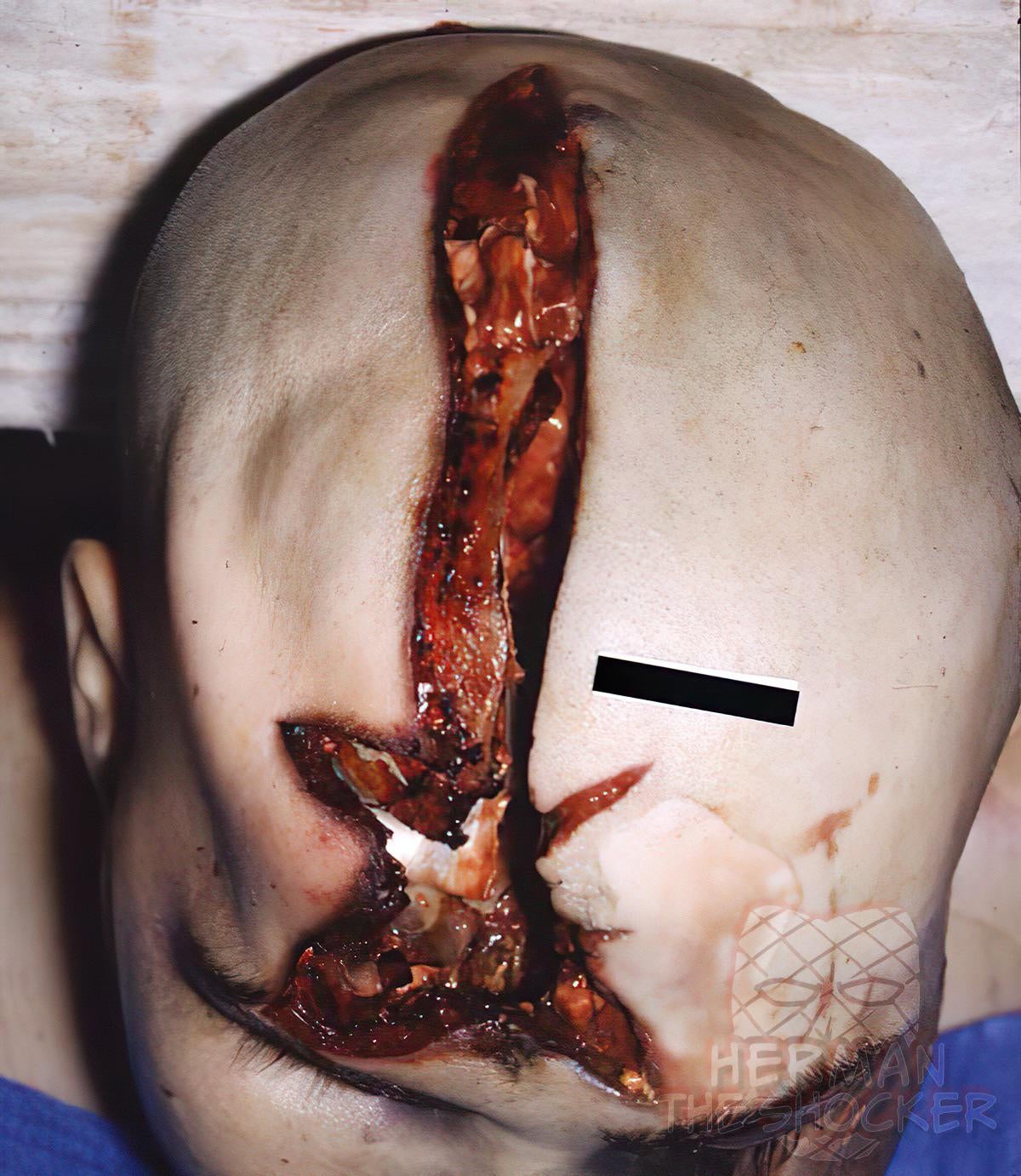 Fig7.1 A gaping stellate wound on the forehead.  Fig7.2 A smaller stellate wound was on the occipitoparietal region. The premise that exit wounds are larger than entrance wounds is a generality only. A man was found in early decomposition on his bed with a rifle next to his body. A gaping stellate wound on the right side of the forehead extended posteriorly to the right parietal region (Fig.1). A smaller stellate wound was on the occipitoparietal region (Fig.2). Examination of the right forehead wound disclosed central blackening of the wound edges, consistent with a contact wound. Examination of the calvarium disclosed external beveling of the edges of the skull wound deep to the occipitoparietal scalp wound, confirming that the posterior, smaller wound was the exit. Skull wounds may be comminuted and, as such, require reapproximation of the bony fragments to allow confirmation of the nature of the beveling. In a contact shot fired anywhere on the head, the gases from the firing discharge can enter into the skull. This results in an acute build-up of intracranial pressure with the rigid cranium attempting to accommodate it by expansion. Gases under pressure accumulate inside the cranium and in the process of attempting to release this build-up of pressure, fractures will arise with outward expansion with outwards pushing of the fracture fragments and consent tears (lacerations) through the skin of the face as these sharp and tough bony fragments are pushed outwards. This is seen especially on the face and this produces facial distortion effects. - Part 1 --- Part 2 --- Part 3 --- Part 4 --- Part 5 --- Part 6 --- Part 7 --- Part 8 --- Part 9 --- Part 10 --- Part 11 --- Part 12 --- Part 13 --- Part 14 --- Part 15 --- Part 16 --- Part 17 --- Part 18 --- Part 19 --- Part 20 --- Part 21 --- Part 22 --- Part 23 --- Part 24 --- Part 25 --- Part 26 --- Part 27 --- Part 28 --- Part 29 --- Part 30 --- Part 31 --- Part 32 --- Part 33 --- Part 34 --- Part 35 --- Part 36 --- Part 37 --- Part 38 --- Part 39 --- Part 40 --- Part 41 --- Part 42 --- Part 43 --- Part 44 --- Part 45 --- Part 46 --- Part 47 --- Part 48 - This post is for educational purposes only and is nonprofit. Under Section 107 of the US Copyright Act of 1976; Allowance is made for "Fair Use" for purposes such as criticism, comment, news reporting, teaching, scholarship, and research. OP is not a medical expert. No copyright infringement intended. This post does not encourage or glorify violence/harassment. Images might have been upscaled and enhanced. Text might have been shortened and simplified/reorganized for online view.
__________________ ⭐️ hermantheshocker.com ⭐️ |
|
#2
●
01-16-2023, 02:25 PM
| ||||||||
| My Rank: FIRST SERGEANT Poster Rank:394 Join Date: Apr 2011 Posts: 3,054 Mentioned: 2 Post(s) Quoted: 276 Post(s)
| ||||||||
|
Re: The Shocker's Mix 49
Once again, a reliable dose of shock therapy |
|
#3
●
01-16-2023, 02:49 PM
| ||||||||
| BEHEMOTH Poster Rank:53 Blue-Eyes White Dragon Join Date: Apr 2021 Posts: 27,692
Contributions: 21
Mentioned: 322 Post(s) Quoted: 13282 Post(s)
| ||||||||
|
Re: The Shocker's Mix 49
Was starting to wonder where you was! Great stuff as always Herman.
__________________ ISRAEL ✔ - PALESTINE ✗ |
|
#6
●
01-16-2023, 04:54 PM
| ||||||||
| ★ Legacy Member ★ Poster Rank:248 So many choices now Join Date: Jul 2015 Posts: 5,548 Mentioned: 15 Post(s) Quoted: 2120 Post(s)
| ||||||||
|
Re: The Shocker's Mix 49
Herm, Case 2: Green Acres TV reboot with a comic sinister twist. Case 6: Handgun acne. |
|
#8
●
01-17-2023, 02:55 AM
| ||||||||
| My Rank: CAPTAIN Poster Rank:214 Join Date: May 2016 Posts: 6,806
Contributions: 21
Mentioned: 3 Post(s) Quoted: 851 Post(s)
| ||||||||
|
Re: The Shocker's Mix 49
Mechanical asphyxia will make a great industrial band name or not |






























{kind=link}