|
#1
●
01-27-2023, 12:32 AM
| ||||||||
| These are the rooms Poster Rank:25 of ruin. Join Date: Sep 2014 Posts: 54,011 Mentioned: 145 Post(s) Quoted: 30403 Post(s)
| ||||||||
|
Granuloma Gravidarium of the Oral Cavity
This is out of India. Source: A 26-year-old prima gravida woman who was 28 weeks pregnant, was referred to the Department of Dentistry for evaluation of a progressively increasing mass in the mandibular teeth region. On examination, a large proliferative gingival growth (approx 5×3 cm) was observed enveloping the occlusal surfaces of all posterior teeth with both buccal and lingual extensions. The lesion was moderately firm on palpation, non-tender and coated with plaque and debris. Some degree of mobility was suggestive of a pedunculated lesion. On manipulation, a sluggish bleed was observed, which however ceased spontaneously in a few minutes. The patient had stopped using a toothbrush for the past several weeks owing to the increased bleeding during tooth brushing. The large lesion was also affecting mastication and speech and bled spontaneously several times a day. Poor oral hygiene with significant materia alba and plaque deposits on all tooth surfaces was recorded. The surface of the lesion had multiple traumatic indentations corresponding to the opposing tooth surfaces (figure 1). A single right submandibular inflammatory lymph node was palpable. The medical history was positive for gestational diabetes mellitus which was managed satisfactorily with insulin therapy. A provisional diagnosis of pregnancy pyogenic granuloma (PG) was made and treatment options were discussed. Although the large lesion and its associated discomfort favoured surgical excision, in view of the advanced pregnancy and the unwillingness of the patient to accept the risks of the proposed surgery, the procedure was deferred until parturition. The patient underwent ultrasonic supragingival scaling to reduce the plaque and calculus deposits, and oral hygiene instructions were reinforced. Chlorhexidine gluconate (0.12%) mouthwash was prescribed to improve oral hygiene and regular follow-up was advocated. The patient reported 8 weeks later for further management of the gingival lesion following intrauterine fetal death 4 weeks earlier. The lesion appeared to show no regression in size or in symptoms. A surgical excision was performed down to the periosteum under general anaesthesia along with extraction of periodontally weakened teeth associated with the gingival growth. The patient withstood the procedure well and the intraoperative and postoperative periods were uneventful. Histological features of prominent endothelial proliferation with capillary formation and associated inflammation confirmed the clinical diagnosis. No recurrence of the lesion was observed at a 2-month follow-up visit.  ·  · 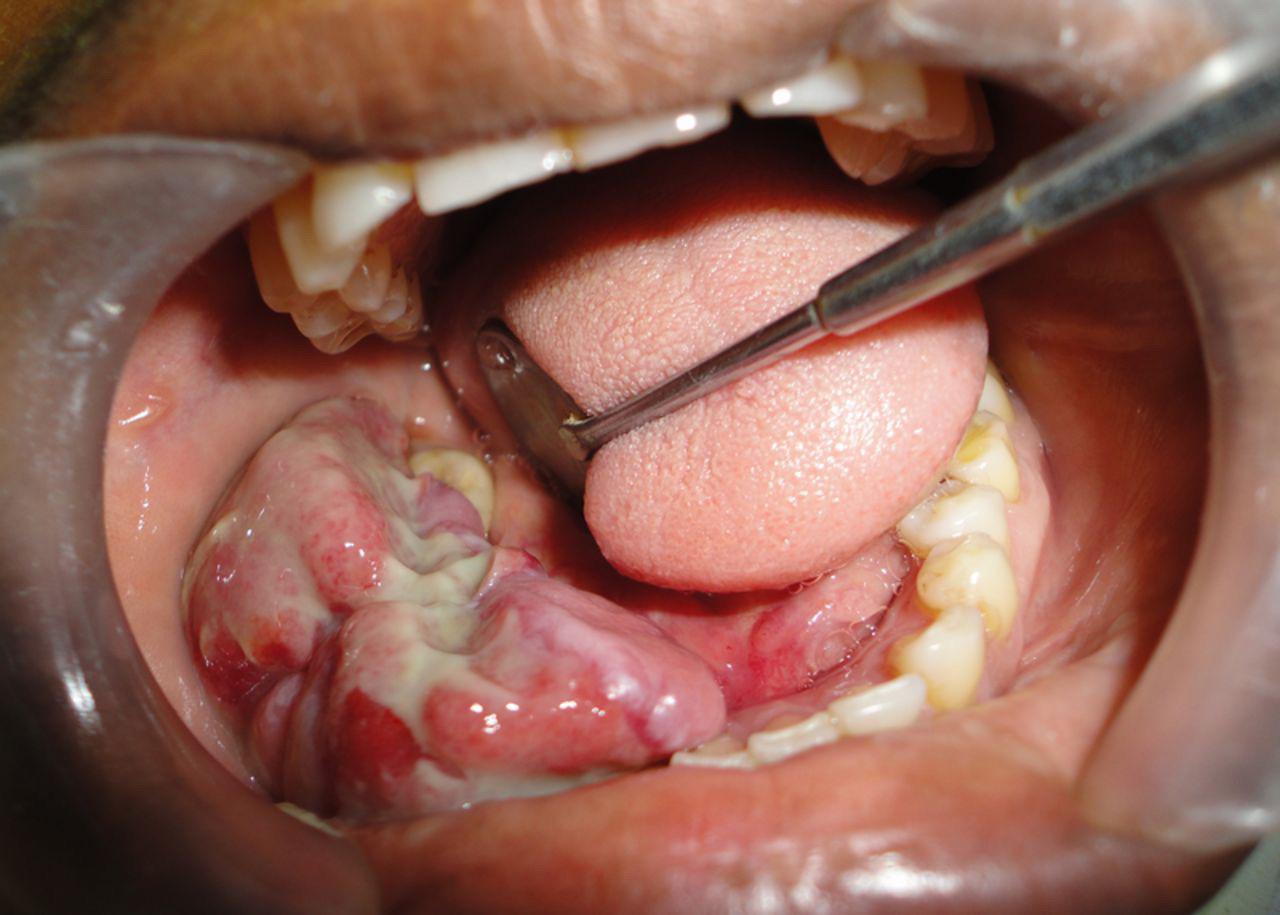 · |
|
#3
●
01-29-2023, 06:14 PM
| ||||||||
| ♚ Legacy Gold Member ♚ Poster Rank:644 Woman Join Date: Apr 2011 Posts: 1,354 Mentioned: 3 Post(s) Quoted: 142 Post(s)
| ||||||||
|
Re: Granuloma Gravidarium of the Oral Cavity
Jesus Christ! I wonder who the dreamer was that knocked her up??! I'll bet between them they could keep a small pharmacy in business!!
__________________ You can not imagine the immensity of the Fuck I do not give. |




















{kind=link}