|
#1
●
04-09-2023, 11:36 PM
| ||||||||
| These are the rooms Poster Rank:25 of ruin. Join Date: Sep 2014 Posts: 54,011 Mentioned: 145 Post(s) Quoted: 30403 Post(s)
| ||||||||
|
Thyroglossal Duct Cyst
Source: A 35-year-old gentleman with a long-standing history of anterior neck swelling for the past 10 years was prompted to seek medical advice when a previously slow-growing neck swelling had rapidly increased in size within four months following a history of fall whereby the anterior neck hit a blunt surface object. However, he did not sustain any external injuries following the incident. The anterior neck swelling remained painless for 10 years, and he did not experience any dysphagia, respiratory distress, or hoarseness. There was also no history of constitutional symptoms and hypo- or hyperthyroidism. He was subsequently referred to our otorhinolaryngology clinic in a tertiary hospital. On examination, he was comfortable with a large anterior neck mass extending superiorly from the mandible until the sternal notch inferiorly (Figure 1). The neck swelling was soft in consistency, non-tender, and smooth on the surface without discoloration of the skin. The mobility on swallowing or tongue protrusion was difficult to be elicited due to the large neck mass. Laryngoscopy using a 70-degree endoscope (Storz®, Germany) was performed, and there was no sign of an airway compromise or compression of the pharyngeal wall from the mass effect of the anterior neck swelling. Laboratory investigation for thyroid function test revealed a euthyroid state. Contrast-enhanced computed tomography (CECT) scan of the neck showed a large, well-capsulated cystic mass measuring 9.3 x 9.0 x 10.7 cm with superior attachment at the body of the hyoid bone (Figure 2a, b). The thyroid gland is present in its usual position. Fine needle aspiration cytology (FNAC) was done and consistent with cystic content without evidence of malignancy. A clinical diagnosis of TGDC was made, and the patient underwent a Sistrunk operation to excise the mass. The mass was completely excised together with the body of the hyoid bone. However, the cyst ruptured during surgical manipulation due to its massive size (Figure 3). The diagnosis of TGDC was confirmed histologically. He recovered well post-operatively with no further recurrence to date (Figure 4). 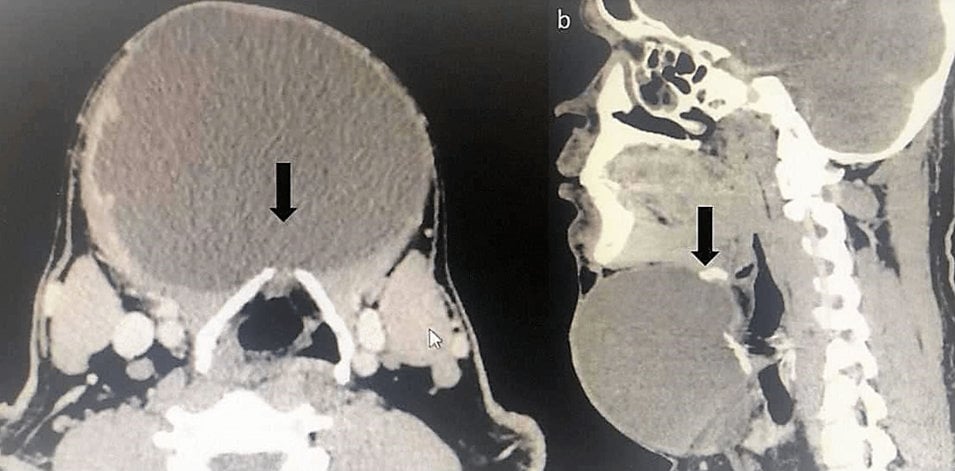 ·  · 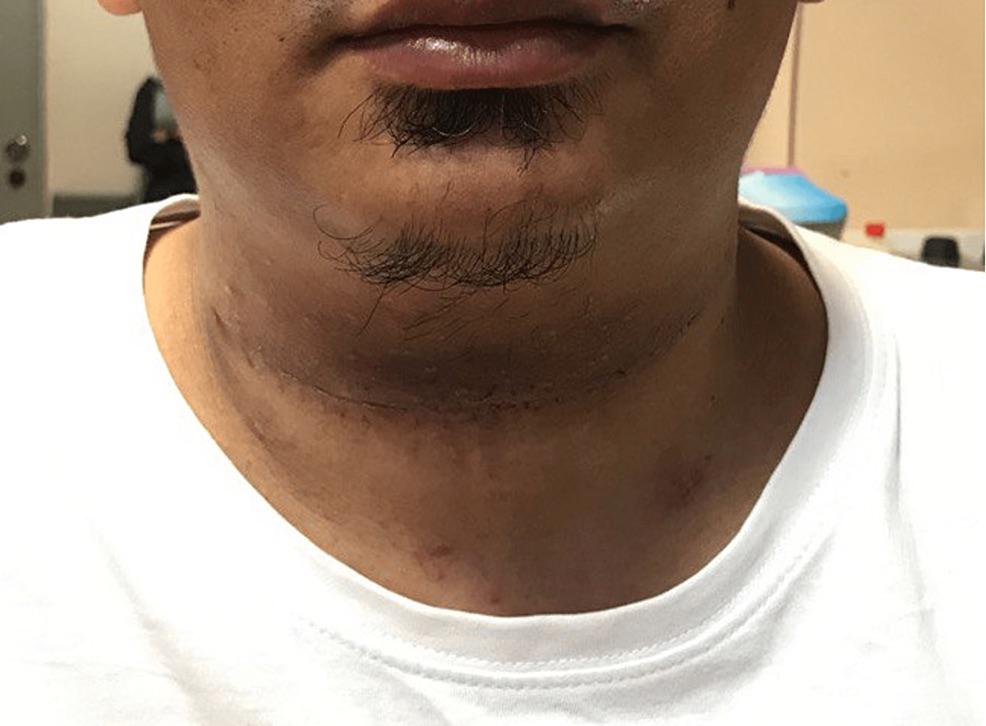 · 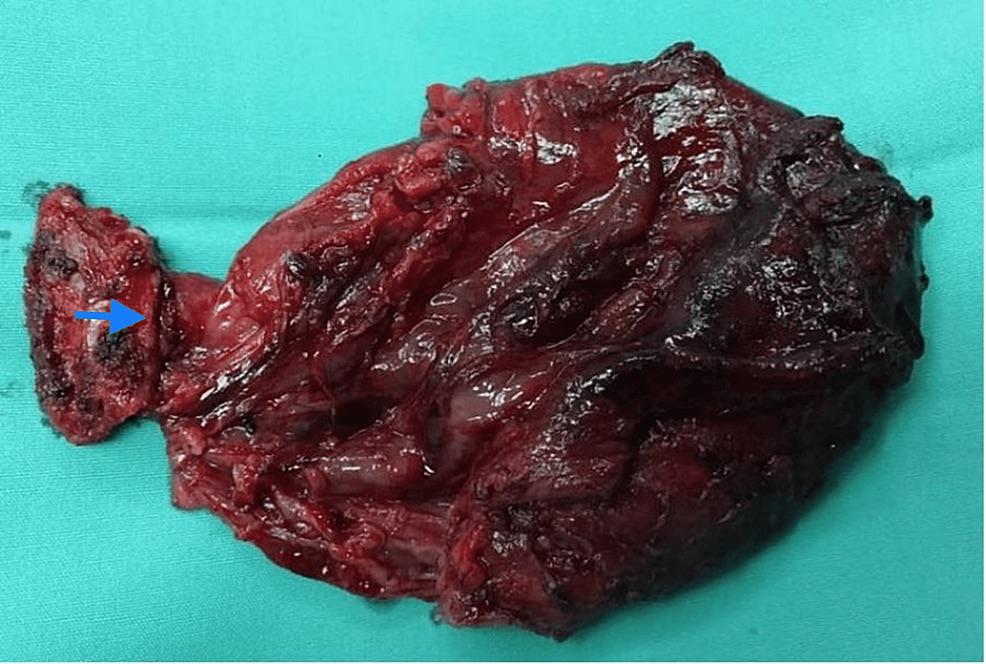 · |
|
#2
●
04-10-2023, 01:42 AM
| ||||||||
| ★ Legacy Member ★ Poster Rank:247 So many choices now Join Date: Jul 2015 Posts: 5,548 Mentioned: 15 Post(s) Quoted: 2120 Post(s)
| ||||||||
|
Re: Thyroglossal Duct Cyst
In certain male birds and frogs, that is a mating call.
|
|
#4
●
04-10-2023, 03:32 AM
| ||||||||
| My Rank: FIRST SERGEANT Poster Rank:393 Join Date: Apr 2011 Posts: 3,054 Mentioned: 2 Post(s) Quoted: 276 Post(s)
| ||||||||
|
Re: Thyroglossal Duct Cyst
In some lizards too. Which makes me ponder how often has he been watching Animal Planet lately? |




























