|
#1
●
09-09-2024, 06:26 PM
| ||||||||
| These are the rooms Poster Rank:25 of ruin. Join Date: Sep 2014 Posts: 54,011 Mentioned: 145 Post(s) Quoted: 30403 Post(s)
| ||||||||
|
Penile Mutilation
A 46-year-old male with a history of paranoid schizophrenia was referred to our hospital after he cut his penile shaft, along with a 3-cm distal part of the mons pubis, with a sharp sickle. Following massive blood loss from the wound, bleeding was controlled after several hours of treatment in a primary health center. The patient also had a history of bloody discharge from the external urethral orifice. After initial evaluation at a tertiary hospital, the patient was admitted to our hospital approximately 3 days after the injury. Following an initial assessment and resuscitation, the patient was administrated tetanus toxoid for prophylaxis and given broad-spectrum antibiotics. Upon admission in the emergency room, mental examination revealed the patient’s apathy, consciousness, and sometimes agitation. The patient’s eye contact was poor, and his speech was incoherent. Urological examination showed a subtotal cut of the penis, including the distal part of the mons pubis and the dorsal and lateral parts of the penile skin, and a clear cut through the corpus cavernosum. The penis remained suspended by only a thin ventral part of the penile skin (Fig. 1). The patient was immediately transferred to the operating room. After the administration of spinal regional anesthesia, the patient was placed in the lithotomy position. Following disinfection and draping, a 16 Fr silicone Foley catheter was carefully inserted into the external urethral orifice. A careful assessment on the penile wound revealed a partial-thickness wound with a relatively well-defined traumatic separation of tissues on the dorsal of the penis, one that crossed the base of the penis and was in fact formed by two incised wounds (Fig. 2A). The first wound caused a 5-cm separation of dorsal of the penis from its base, whereas the second wound was located more proximally from the first and separated the penis about 3 cm from its base. The transection of the corpus cavernosum and corpus spongiosum was discovered along with a 1-cm defect of the bulbous urethra (Fig. 2B). We assessed the wound as Grade IV penile injury according to the American Association for the Surgery of Trauma (AAST), because although the urethral defect was less than 2 cm, the cavernous defect exceeded 2 cm. Once surgery was planned following a multidisciplinary approach, the patient was transferred to the operating room 2 h after arriving at the emergency department. We (i.e., a urologic surgeon and general surgery resident) performed a debridement procedure and refreshed the wound edge (Fig. 3A). The corpus cavernosum was re-anastomosed with an interrupted suture using absorbable polyglactin 5/0 (Fig. 3B). Next, the defect of the bulbous urethra was closed, also with an interrupted suture using absorbable polyglactin 5/0. We did not perform any anastomosis of the dorsal vein, artery, or nerve. After deep (Buck’s) and superficial (Dartos) fascia were reapproximated (Fig. 3C), the operation was finished with another interrupted suture of the skin. A Penrose drain was left on each of the right and left sides of the wound (Fig. 3D). After acute surgery, the patient was transferred to the psychiatric department for the management of his psychiatric condition. Intravenous antibiotic ampicillin–sulbactam was administered 3 times daily. After leaving the psychiatric department, the patient received antipsychotic risperidone (2 mg, twice daily) and clozapine (25 mg, once daily). Proper wound care was performed every 2 days to investigate the wound’s condition and to ensure successful wound healing. On Day 3 postsurgery, the Penrose drains were removed, and on Day 6, the patient was discharged from the hospital. His surgical wound had recovered well, and neither skin necrosis nor infection was observed (Fig. 4). The silicone Foley catheter was maintained for another 21 days. Approximately 4 weeks postsurgery, the Foley catheter was removed, and the patient appeared to have recovered well and was urinating effectively without any symptoms of urethral stricture. The entire penis remained viable with minimal scarring at the surgical site and could achieve and maintain erection. 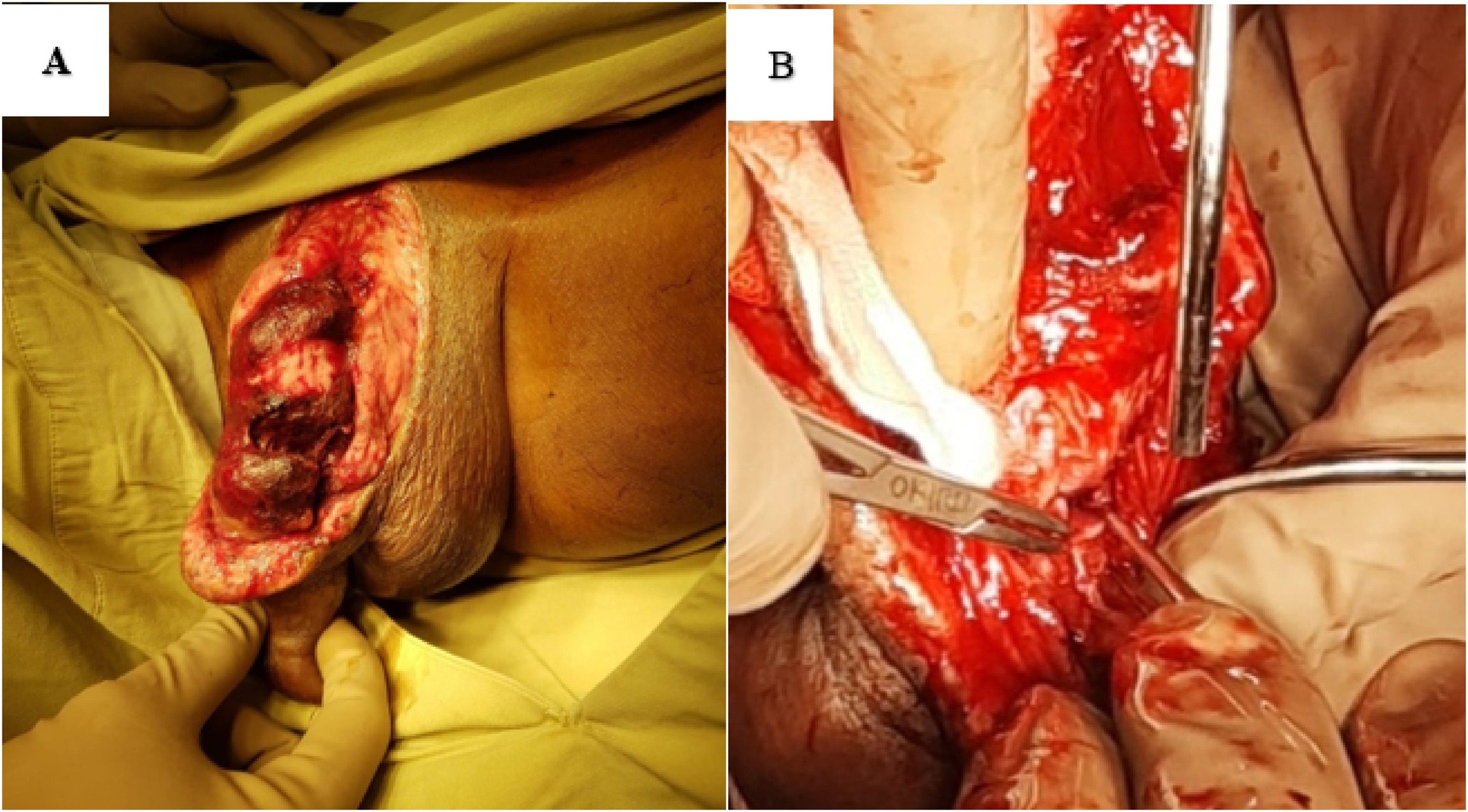 ·  · 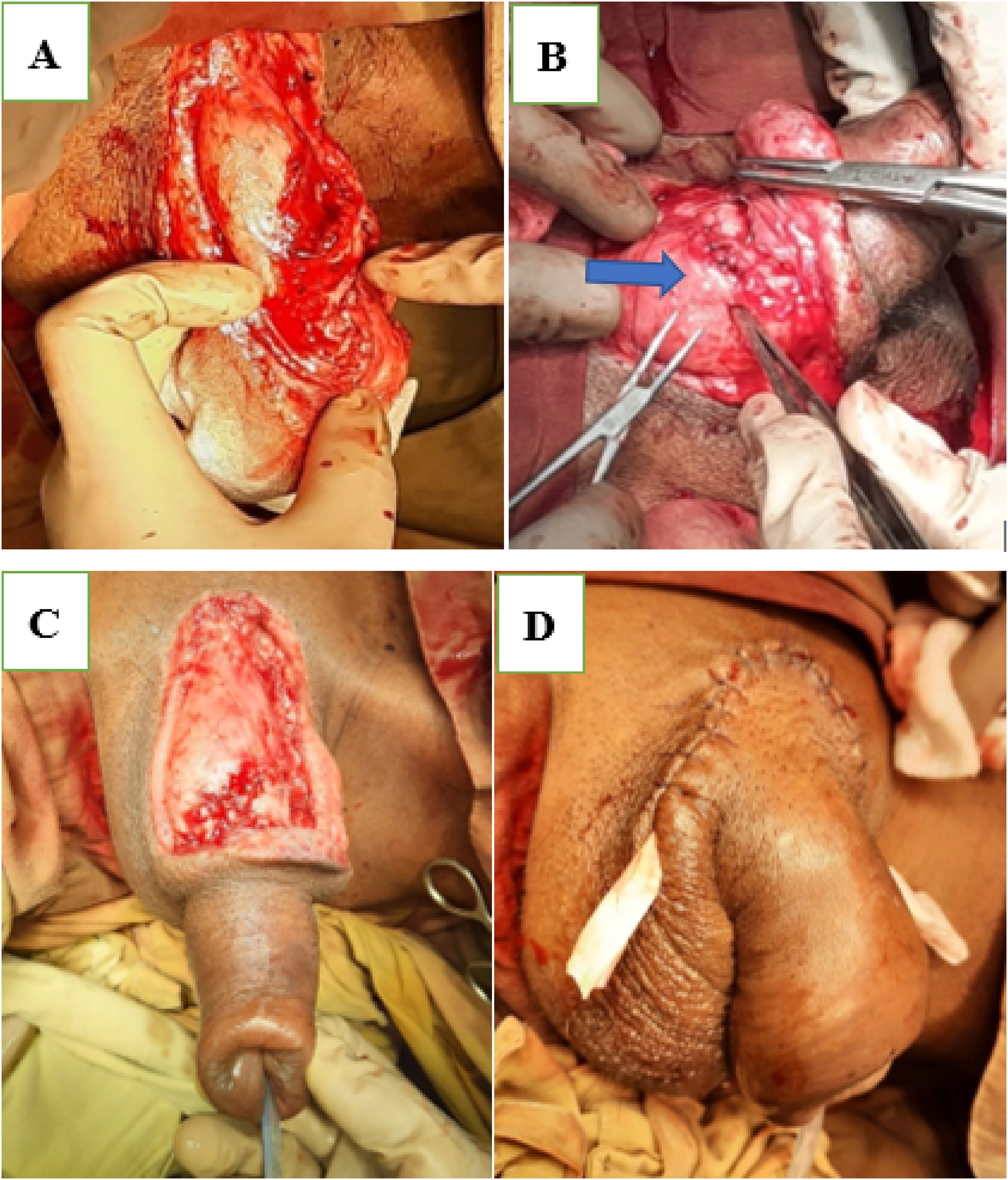 ·  · |
|
#2
●
09-09-2024, 11:38 PM
| ||||||||
| My Rank: MASTER GUNNERY SERGEANT Poster Rank:347 Manly Man Join Date: Sep 2017 Posts: 3,601 Mentioned: 0 Post(s) Quoted: 700 Post(s)
| ||||||||
|
Re: Penile Mutilation
This man doesn't deserve to have a penis.
|


















