|
#1
●
08-07-2024, 04:48 PM
| ||||||||
| These are the rooms Poster Rank:25 of ruin. Join Date: Sep 2014 Posts: 54,011 Mentioned: 145 Post(s) Quoted: 30403 Post(s)
| ||||||||
|
Keratoderma
The patient presented as a five-year-old female with no prior medical problems except those related to her PPK as can be seen in Figure 1 and Figure 2. The patient had been actively seen by Dermatology Department, who were attempting to decrease her PPK to the point where it was manageable. Three years prior to getting surgical management, the patient had been admitted multiple times due to severe infection with systemic complications and sepsis. Her feet were also painful and were treated for intractable pain. The patient was confined to a wheelchair. The patient had tried multiple topical treatments and soaks with no improvement. Areas of cracking, pain, and infection were present on her first visit. Debridement was initially discussed. The patient had some debridement done sharply, but the keratoderma subsequently thickened rapidly. Deeper debridement was presented as an option. With the use of the harmonic scalpel and a smoke evacuator debridement was carried out into the deep portions of the dermis as can be seen in Figure 3. Initially, this was an effective procedure, allowing the patient to remain without thickened changes, infection, smell, or pain for approximately 3 to 4 months. Several of these debridement procedures were done. Approximately 3 to 4 months after the last debridement, recurrence was rapid as can be seen in Figure 4. The patient who had been able to walk was again wheelchair bound. The decision was made to excise the keratoderma en bloc, removing the dermis and subcutaneous tissue, as shown in Figure 5. The excised tissue can be seen in Figure 6, which reveals the plantar fascia of the feet. After excision, Integra would be placed with negative pressure wound therapy (NPWT), followed by a second layer of Integra with NPWT, allowing for a more durable sole of the foot. Final coverage would be achieved with a thin split-thickness graft, as shown in Figure 7. The risks and complications of this aggressive treatment were understood, and one foot was operated on first. The surgery went successfully, and the patient was able to bear weight after the skin graft fully healed. Attention was then turned to the other foot, which was also successfully treated in the same fashion. With success noted in the feet, attention was turned to the hands, starting with the right hand. The procedure was done in a similar fashion, down to the palmar fascia, and extending to the subcutaneous tissue of the fingers. Great care was taken not to damage digital arteries or nerves. The patient’s fingers were pinned straight to decrease the possibility of contracture. After NPWT and granulation, a thin split-thickness skin graft was placed as can be seen in Figure 8. This procedure was repeated for the contralateral side. The patient was monitored carefully. Some areas of minimal recurrence were noted, less than 1 cm (about 0.39 in) in diameter and were treated with wound care with topical urea. When one area did progress, a small resection was done followed by skin grafting. After six months of walking as a middle school student, there was breakdown of the heel to the plantar fascia. Concern for osteomyelitis and progression of the wound prompted the use of a rectus free flap to allow for significant padding in this portion of the heel followed by a conventional split-thickness skin graft. The flap was monitored appropriately and shrank with no recurrence. After 16 years, the patient now walks and is currently a college student with the stability of her hands as can be seen in Figure 9 and feet as can be seen in Figure 10. She is able to take notes and type, with an almost full range of motion of her fingers. The patient states that she is able to lead a normal and productive life.  ·  ·  ·  ·  · 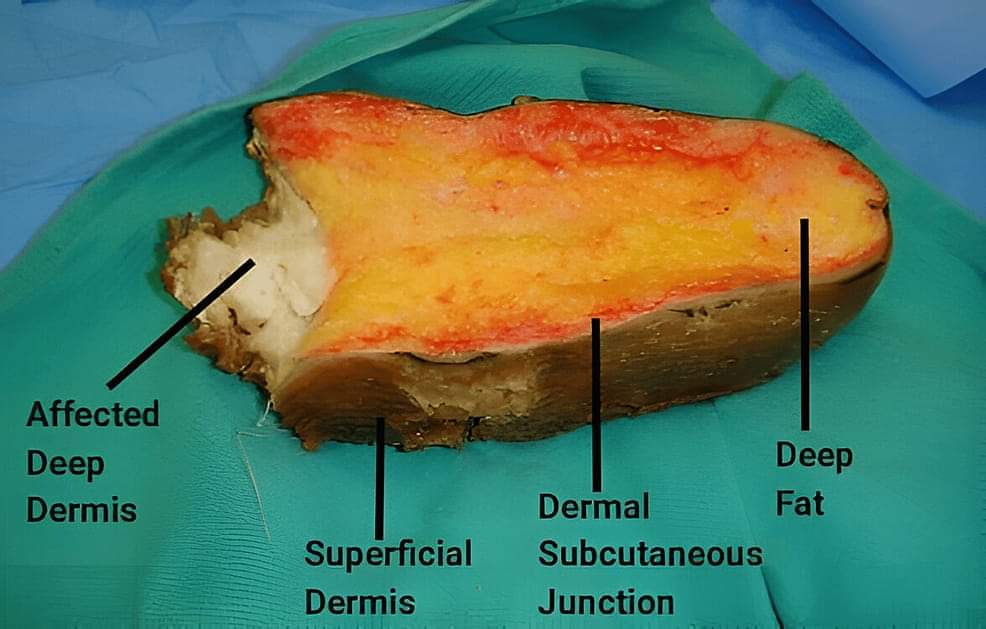 ·  ·  ·  ·  · |
|
#4
●
08-08-2024, 09:10 PM
| ||||||||
| My Rank: CORPORAL Poster Rank:1285 female Join Date: May 2009 Posts: 474 Mentioned: 0 Post(s) Quoted: 35 Post(s)
| ||||||||
|
Re: Keratoderma
All of this seems like medical experiments. Are humans that special we need them ( us ) all. Hardly .
|






















