|
#1
●
01-17-2023, 10:20 PM
| ||||||||
| These are the rooms Poster Rank:25 of ruin. Join Date: Sep 2014 Posts: 54,011 Mentioned: 145 Post(s) Quoted: 30403 Post(s)
| ||||||||
|
Twisted Ovarian Dermoid Cyst During Pregnancy
Source: A 23-year-old primigravida presented to the ANC clinic with severe, non-radiating, unrelieved abdominal pain and four episodes of vomiting for four hours. Her symptoms were severe and unrelieved by medication, and she had no history of vaginal discharge or bleeding. The patient conceived naturally without treatment and provided no information about any illnesses, fevers, urinary problems, diarrhea, or constipation. The patient had one visit at eight weeks of gestation and had no relevant medical or surgical history. On general examination, her blood pressure was 90/60 mmHg, pulse rate was 112/min, afebrile, and her cardiovascular and respiratory systems were normal. A tender adnexal cystic mass was detected on abdominal examination, in addition to a 14-week palpable uterus. These findings were corroborated by vaginal examination. All of her blood and urine test results were within normal limits. Ultrasonography revealed a 14 cm × 11 cm single mass lesion in the left iliac fossa with thin-walled septa and dermoid cyst components. It also showed a single intrauterine live fetus of 14 weeks with a placenta developing in the fundoposterior segment. With proper consent and in view of an acute emergency patient was posted for emergency laparotomy under spinal anesthesia after giving a stat dose of intramuscular synthetic hydroxy progesterone, 500 mg. A right ovarian cyst measuring 14 cm x 10 cm was visualized to be triply rotated around its pedicle, as shown in Figure 1. Oophorectomy was done immediately after untwisting it. A histopathological examination was requested for the cyst, contents are shown in Figure 2. The other ovary was found to be normal. The procedure was uneventful. The patient was kept on Intravenous tocolytics for first postoperative day followed by oral tocolytics 10 mg twice a day for 14 days. A normal postoperative obstetric ultrasound suggesting live 15 weeks fetus was observed on the ninth postoperative day when the patient was discharged. Being a vertical scar and far-stay, the patient was willing to stay till suture removal. The patient is being monitored regularly and the fetus is healthy and growing well. The resected dermoid cyst of the ovary was diagnosed on the basis of the histopathological examination showing keratinizing, stratified squamous epithelial lining, intraluminal keratin, hair and sebaceous glands. 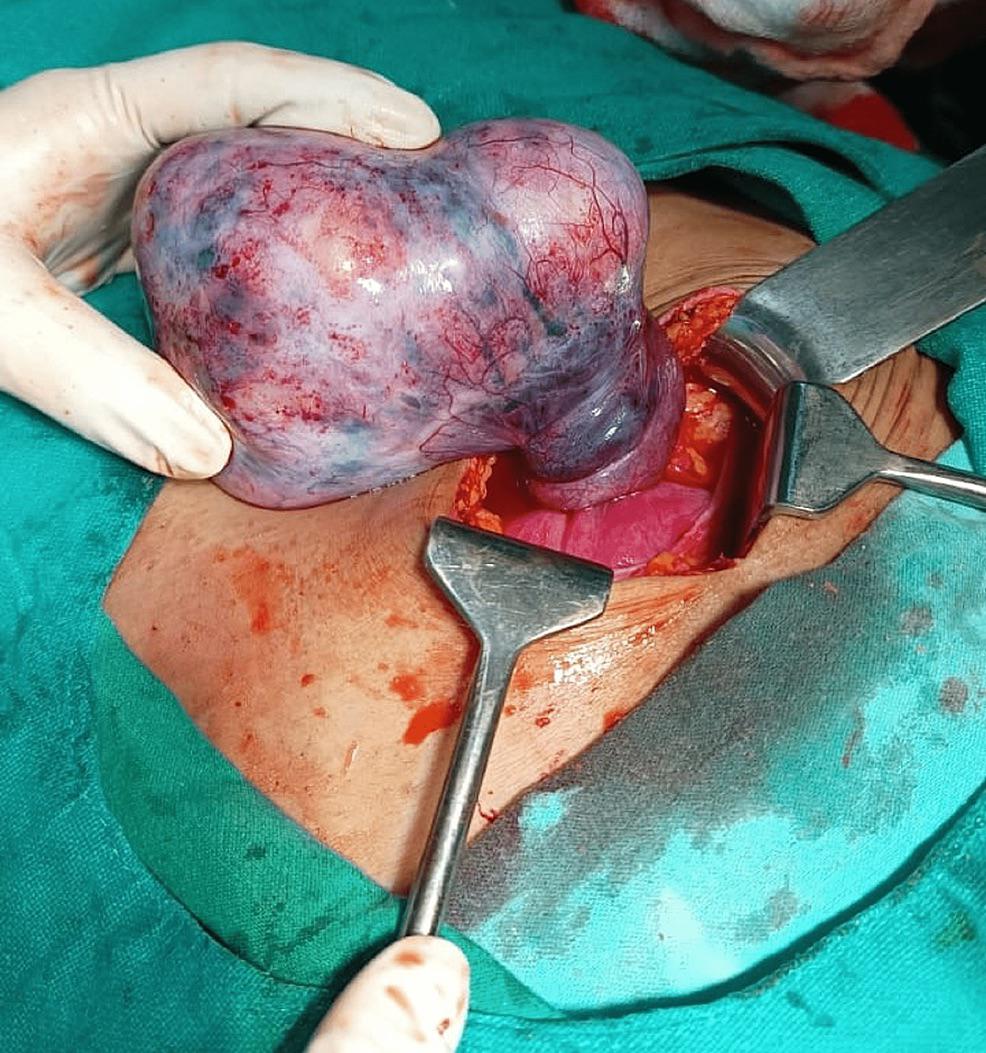 ·  · |
|
#2
●
01-18-2023, 12:34 AM
| ||||||||
 ★ Legacy Member ★ Poster Rank:772 I'm not A bitch.... I'm THE bitch. Join Date: Jul 2012 Posts: 1,034 Mentioned: 4 Post(s) Quoted: 174 Post(s)
| ||||||||
|
Re: Twisted Ovarian Dermoid Cyst During Pregnancy
Yummy........ They're awesome outside the body, but look cooler coming from the inside. |
















{kind=link}