|
#1
●
07-13-2021, 01:21 PM
| ||||||||
| ♚ Legacy Gold Member ♚ Poster Rank:907 Join Date: Jul 2020 Posts: 820
Contributions: 10
Mentioned: 13 Post(s) Quoted: 173 Post(s)
| ||||||||
|
Sub-decapitation in Suicidal Chainsaw Injury
Chainsaw accidents are severe injuries, mostly work-related and concerning upper or lower extremities. Few suicidal chainsaw injuries are reported, all of them fatal. We report the case of a 23-year-old man who attempted suicide by sub-decapitation with a chainsaw, its successful (peri-) operative management, and clinical course along with a discussion of the contemporary management and body of evidence of such lesions. Chainsaw injuries are severe traumas. Stepwise surgery with maximal functional reconstruction is safe and optimal clinical outcomes can be achieved.  Fig.1 Top: cervical trauma at admission; bottom: scaring 3 weeks after surgery. 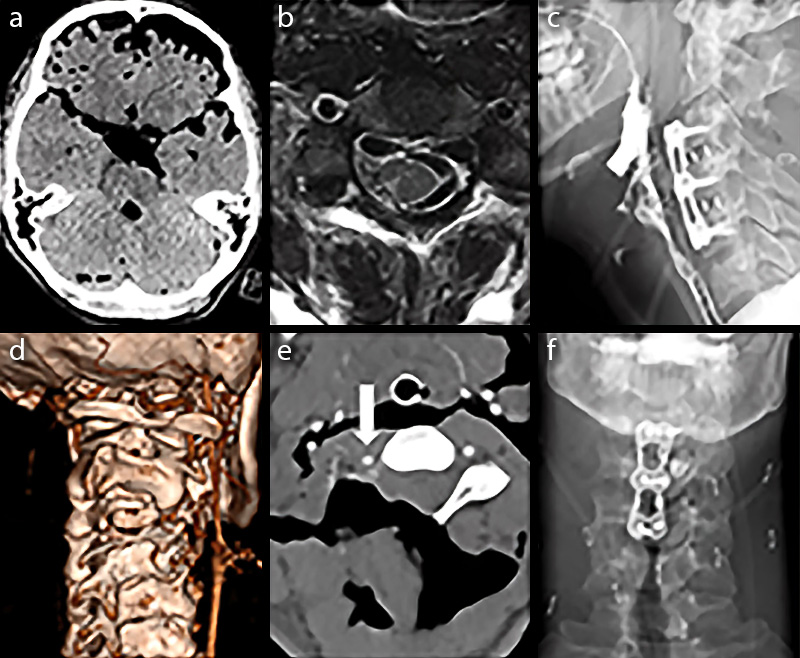 Fig.2
History and examination The evening before admission, the patient tried to perform suicide by auto-decapitation using a chainsaw and was found by his brother the following morning. At the site of injury, the emergency physician encountered a patient with stable circulation and a GCS of 13 without motor deficits (Fig. 1). On-site intubation, cervical spine immobilization was immediately performed and the patient was transferred to the emergency department of a tertiary care hospital in southern Germany. On arrival, the patient presented in stable conditions with pupils equally round and reactive to light. The extensive cervical trauma was covered with sterile bandages without signs of further traumatic lesions. Neuroimaging Trauma computed tomography + angiography head/neck emergency room (ER): Severe soft tissue trauma of the cervical muscles with arrosion of the right C3 hemilamina and partial arrosion of the C4 inferior articular process. Extensive pneumatic infiltration of intra- and extradural cranium and spine. Major vascular structures (carotid and vertebral arteries) intact (Fig. 2). Whole spine magnetic resonance imaging (MRI) (postoperative): Small right-side ischemic lesion of the spinal posterior column. No further radicular, spinal cord, or brain lesion (Fig. 2). Cervical spine X-ray/barium swallow (postoperative): Esophagus intact without fistula. Appropriate placement of cages and plate (Fig. 2). Surgery First, a cerebrospinal fluid (CSF) drainage was inserted into the right frontal horn of the lateral ventricle for intracranial pressure (ICP) monitoring and support dural sealing through CSF diversion. Then, the patient was placed in a prone position with the head fixated in a Mayfield clamp. An extensive cervical wound (including contamination by textile fibers) debridement and closure of the dural laceration was performed using a TachoSil®(Takeda Pharmaceutical, Tokyo, Japan) in/onlay technique with additional fluid sealant DuraSeal®(Integra LifeSciences, Plainsboro, USA) application. No primary closure was possible due to the extensive dural defect. The remaining right C3 hemilamina was resected and numerous cervical myotomies were reconstructed. An anterior cervical soft tissue reconstruction including inspection of trachea and esophagus was performed after transfer to a supine position in the same surgery. The patient was then transferred to the intensive care unit (ICU) with external cervical spine immobilization and ICP monitoring under continuous sedation. The following day, an anterior cervical discectomy and fusion C3/4/5 with ventral plating was performed. Postoperative course After surgery, the patient was continuously monitored at our neurosurgical ICU with repetitive neurological examinations. Anti-infective therapy with vancomycin, meropenem, and metronidazole was administered until the fifth postoperative day (POD) and continued with vancomycin and meropenem until POD 14. At POD 3, extubation was performed followed by immediate psychiatric care. The patient showed hypesthesia of the right IV and V fingers without further sensorimotor deficits. At POD 14 without signs of surgical site infection, the patient was transferred to the psychiatry department to continue the treatment for major depression. Discussion Comprehensive analysis for the management of open cervical trauma does not exist to date. In case of extensive cervical trauma, securing the airway is of the highest priority followed by cervical spine immobilization and sterile wound coverage. In the case of vascular lesions, hemostasis should be assured in the preclinical setting. Corresponding to open fractures, anti-infective prophylaxis should be initialized as soon as possible using second-generation cephalosporine. In this case, due to major dural laceration, the prophylaxis was extended to the CNS penetrating antibiotics. In open cervical trauma, surgical exploration, debridement, and anatomical reconstruction should be performed on the same day. Peripheral nerve reconstruction can be performed during the same session or at a later time point. A dural laceration is accompanied by a raised perioperative complication rate and can lead to meningitis, insufficient wound healing, pseudomeningocele, intracranial hypotension, or subdural hematoma. Traumatic dural lacerations do not show substantial differences compared with iatrogenic lesions regarding management and complication rates and its treatment comprises conservative management, primary closure with sutures, fibrin glue, biological sealant patches, CSF diversion, or a combination. Clear evidence demonstrating the superiority of either technique or material is still lacking. Surgical management of the spinal bony structures has to be chosen taking into account spinal stability, the characteristics of injury, and the presence or absence of spinal stenosis. In the case presented here, no clear guidelines are applicable. If primary dorsal, anterior, or a 360° fusion should be favored is controversially discussed. If choosing an anterior approach, a cage-plate combination is the most widely accepted technique. In the present case of an unstable cervical spine along with altered anatomy of the dorsal structures, a two-level anterior approach with discectomy, cage, and ventral plate the day after trauma was chosen. P. Krauss, V. M. Butenschoen, B. Meyer, & C. Negwer - May 2020. Department of Neurosurgery, Klinikum rechts der Isar, Ismaninger Strasse 22, 81675 Munich, Germany. - This post is for educational purposes only and is nonprofit. Under Section 107 of the US Copyright Act of 1976; Allowance is made for "Fair Use" for purposes such as criticism, comment, news reporting, teaching, scholarship, and research. OP is not a medical expert. No copyright infringement intended. This post does not encourage or glorify violence/harassment. Images might have been upscaled and enhanced. Text might have been shortened and simplified/reorganized for online view. |
|
#2
●
07-13-2021, 05:48 PM
| ||||||||
| ★ Legacy Member ★ Poster Rank:247 So many choices now Join Date: Jul 2015 Posts: 5,548 Mentioned: 15 Post(s) Quoted: 2120 Post(s)
| ||||||||
|
Re: Sub-decapitation in Suicidal Chainsaw Injury
Chainsaw suicide? My new punk band name. On a more practical note, I'd be thinking that is a non-starter in terms of suffering. Not a Q&D solution. Hear me out - it doesn't matter how you approach the neck, your arms and hands are trying to hastily guide the saw to the target area at maximum RPM and chain speed, but with arms bent and-or outstretched at very odd angles. Once you get to the point of the chain actually biting into flesh, your instinct, no matter what your intended outcome, is to try and stop the pain as quickly as possible, no matter that you are actually trying to off yourself. Trigger is instantly released and hands go to the very spot you are trying to cut. All control of the saw is quickly abandoned, and it's gonna cut into whatever is in the bar's path of travel towards the floor. Added bonus, the reduction of speed in the chain's trip around the bar will result in increased ripping of flesh rather than a clean high speed cut. Result? A jagged scar and a cool story to tell to the folks in the support group. 0/5 would not recommend. |
|
#3
●
07-13-2021, 07:29 PM
| ||||||||
 My Rank: GUNNERY SERGEANT Poster Rank:625 Join Date: Aug 2017 Posts: 1,427 Mentioned: 0 Post(s) Quoted: 262 Post(s)
| ||||||||
|
Re: Sub-decapitation in Suicidal Chainsaw Injury
How in the hell did he survive that? |
|
#6
●
07-16-2021, 04:10 PM
| ||||||||
| ♚ Legacy Gold Member ♚ Poster Rank:194 Female Join Date: Nov 2009 Posts: 7,754 Mentioned: 5 Post(s) Quoted: 706 Post(s)
| ||||||||
|
Re: Sub-decapitation in Suicidal Chainsaw Injury
D and E in the info. No major arteries cut. |
|
#7
●
07-17-2021, 12:59 AM
| ||||||||
| ★ Legacy Member ★ Poster Rank:320 Female Join Date: Jul 2009 Posts: 4,000 Mentioned: 2 Post(s) Quoted: 6 Post(s)
| ||||||||
|
Re: Sub-decapitation in Suicidal Chainsaw Injury
Well thanks, that answered my question. For some reason I am curious to know just how much the total bill was; between all the surgeries, meds and physical rehab. Thinking maybr in the high six to low 7 figures. |
|
#8
●
07-17-2021, 05:40 PM
| ||||||||
| ♚ Legacy Gold Member ♚ Poster Rank:907 Join Date: Jul 2020 Posts: 820
Contributions: 10
Mentioned: 13 Post(s) Quoted: 173 Post(s)
| ||||||||
|
Re: Sub-decapitation in Suicidal Chainsaw Injury
Probably not much, since it happened in Germany, just a few euros.
|
|
#9
●
07-18-2021, 01:34 AM
| ||||||||
| ★ Legacy Member ★ Poster Rank:320 Female Join Date: Jul 2009 Posts: 4,000 Mentioned: 2 Post(s) Quoted: 6 Post(s)
| ||||||||
|
Re: Sub-decapitation in Suicidal Chainsaw Injury
Thanks Shocker. Never even occured to me where this happened. (Derp!)
|
|
#10
●
07-22-2021, 11:29 PM
| ||||||||
| My Rank: LANCE CORPORAL Poster Rank:2350 Join Date: May 2013 Posts: 194 Mentioned: 0 Post(s) Quoted: 60 Post(s)
| ||||||||
|
Re: Sub-decapitation in Suicidal Chainsaw Injury
That's amazing. Firstly that he had no motor deficits despite the spinal injuries... secondly that he was found the next morning alive and hadn't bled out (if he'd started sawing from the front/throat, and severed arteries first.. he'd be dead)... and thirdly that is one fucking weird arse angle to decide to saw ones own head off. I wonder how he set it up? I've never used a chainsaw for anything but imagine it would be very awkward and you'd want it running and held by something that would lower the chainsaw down onto you so you have no control/escape once its in motion? Like a guillotine? I'm so curious. |


























