|
#1
●
09-26-2024, 05:10 PM
| ||||||||
| These are the rooms Poster Rank:25 of ruin. Join Date: Sep 2014 Posts: 54,011 Mentioned: 145 Post(s) Quoted: 30403 Post(s)
| ||||||||
|
Silicone Pneumonitis
A nonsmoker 55-year-old woman was admitted in our hos-pital for dyspnea associated with intermittent fever up to 38°C. These symptoms had been present for a few months during effort, then also at rest. Her medical history consisted of primary hyperparathyroidism under pharmacological therapy and no allergies. Besides she reported many breast silicone injections for aesthetic purposes ~25 years before. The clinical examination of the thorax showed the presence of an extended breast scarring bilaterally, a complete deformity of the breast cone with nipple-areola complex herniation and a hard-full-thickness scar tissue with many subcutaneous nodules, observed through palpation of the remaining breast tissues (Fig. 1). Spirometry exam showed values compatible with a pul-monary restrictive syndrome. Chest X-ray investigation did not reveal any abnormality. The subsequent computer tomography scan excluded any sign of pulmonary embolism or infectious pneumonitis but it showed an interstitial lung disease, with a reticular fibrosis pattern, and several traction bronchiectasis. No lymphadenopathies or pleural effusion was noticed. Breast tissues showed an important and dishomogeneous increase in thickness with presence of hyper-dense nodules of silicone (Fig. 2). The ultrasound study of axillary nodes displayed a similar bilateral pattern with lymph nodes fulfilled with foreign material. The bronchoscopy procedure with analysis of the bronchoalveolar fluid showed the presence of alveolar macrophages with intra-cytoplasmatic deposits of foreign particulate material, bire-fringent in polarized light. Subsequent immunologic tests excluded any autoimmune disease. The patient was then treated for 10 days with oxygen therapy, beclomethasone, salbutamol, and broad-spectrum antibiotic therapy. In agreement with pulmonologists' diag-nosis of a restrictive syndrome due to the thoracic extensive scarring tissue and the high demand of oxygen therapy, we planned an extensive surgical removal of the scarring tis-sue. We also planned a simultaneous reconstruction with a deep inferior epigastric perforator flap (Fig. 3) because of the wide bilateral involved area and the possibility of sternal exposure. The debridement was performed involving also part of the muscular plane that was broadly filled with liquid silicone (Fig. 4). The flap was harvested bilaterally based on a preoperative computed tomography angiography to determine the exact position of perforators (Figs. 5A and 5B). The deep inferior epigastric artery was anastomized with the thoracodorsal artery, the same for the two comitantes veins. During the operation, we observed venous congestion. Therefore, we decided to perform two additional anastomoses between the superficial epigastric and the lateral thoracic veins. At the end of the procedure, four drains were positioned: two in the donor site and one for each breast. The patient was transferred in the intensive care unit department for the first 48 postoperative hours and a heater lamp was applied above the flap. The flap was monitored through handheld Doppler every hour and observing capillary refill and temperature. Low molecular weight heparin and broad-spectrum antibiotic medication (cefazolin 1 g thrice daily [TID]) were administered for the first 10 days. Analgesic covering was reached using paracetamol 1 g TID and ketoprofen 10 mg twice daily. After 48 hours, the patient was transferred to the plastic surgery department where she was maintained at rest until the fifth postoperative day. Drains were removed completely after 8 days with a fluid output lower than 20cc each. The patient was discharged 10 days after the procedure. A compressive abdominal girdle was applied and physical activity was avoided for 6 weeks (Fig. 6). 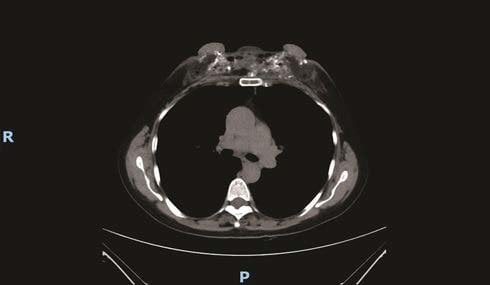 ·  ·  ·  · 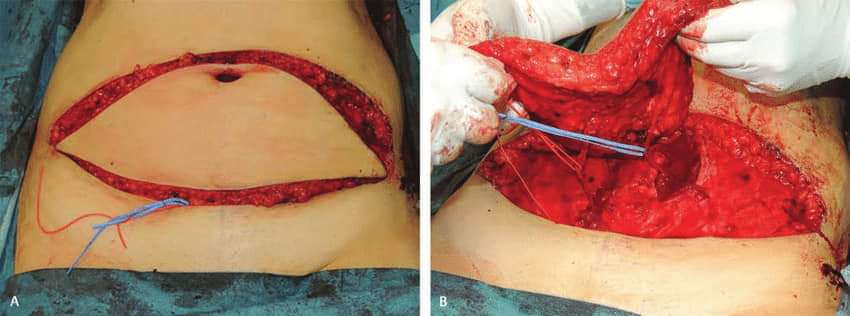 ·  · |
|
#2
●
09-27-2024, 12:41 AM
| ||||||||
| ★ Legacy Member ★ Poster Rank:119 Secret Agent Join Date: Dec 2009 Posts: 13,206 Mentioned: 6 Post(s) Quoted: 2787 Post(s)
| ||||||||
|
Re: Silicone Pneumonitis
Holy fucking hell!! Those first photos… |
|
#5
●
09-27-2024, 05:25 AM
| ||||||||
| ♚ Legacy Gold Member ♚ Poster Rank:553 your supreme lord & master Join Date: Apr 2017 Posts: 1,803 Mentioned: 2 Post(s) Quoted: 354 Post(s)
| ||||||||
|
Re: Silicone Pneumonitis
Picture 2 looks like the buttons on my dining room chairs.
|
|
#6
●
09-27-2024, 01:25 PM
| ||||||||
| My Rank: PRIVATE FIRST CLASS Poster Rank:3685 Female Join Date: Aug 2022 Posts: 91 Mentioned: 1 Post(s) Quoted: 16 Post(s)
| ||||||||
|
Re: Silicone Pneumonitis
I'm dead ass laughing so hard. They do look like buttons |
|
#7
●
09-27-2024, 07:07 PM
| ||||||||
 My Rank: PRIVATE Poster Rank:7964 Old Female Join Date: Jul 2024 Posts: 23 Mentioned: 0 Post(s) Quoted: 7 Post(s)
| ||||||||
|
Re: Silicone Pneumonitis
I'll keep my old saggy boobs any day of the week. And so will my husband.
|
































