|
#1
●
03-15-2023, 09:30 PM
| ||||||||
| These are the rooms Poster Rank:25 of ruin. Join Date: Sep 2014 Posts: 54,011 Mentioned: 145 Post(s) Quoted: 30403 Post(s)
| ||||||||
|
Rectal Issues.
Source: A 61-year-old man with a three-day history of painful swelling around his perirectal area after enema application was referred to our clinic. He expressed the anal pain was precipitated by the first application of enema. He was preparing for colonoscopy for routine colorectal cancer screening program. His medical history was unremarkable. At admission, his vital signs were normal except a slight fever (37.6°C). On physical examination, painful fluctuating abscess located at the left lateral wall of the anus was observed. On digital examination, more than a half of the posterior wall of the rectum had perforated. His abdominal examination was normal. Laboratory parameters revealed mild leukocytosis (14,200/mm3) and increased C-reactive protein (72 mg/dL). Abdominal CT demonstrated the presence of a left posterolateral rectal abscess extending to the mesorectum compatible with an extraperitoneal rectal injury. On sigmoidoscopy, the perforation started from 2 cm above the dentate line extending up to 10 cm along the rectum with a diameter of 10 cm and a depth of 3 cm (Figure 1). The pouch was irrigated with saline. Because of the size, fragility and tightness of the injured tissue, over-scope clip was determined to fail to close the defect. Hence, the surgery was planned. On surgery, perianal abscess drainage and laparoscopic sigmoid loop colostomy was performed. Subsequently, a 10 cm-long modified VAC sponge was placed into the cavity via colonoscopy and the system was continuously set at -40 mmHg. After the procedure, the patient completed five days course of oral ciprofloxacin 500 mg every 12 hours and metronidazole 500 mg every eight hours. The inflammatory parameters decreased after postoperative Day 2. The drainage system was renewed every 72 hours for three times. The system was well-tolerated by the patient. The postoperative course was uneventful. The patient was discharged after removing the system on postoperative Day 10. The rectum was checked by both sigmoidoscopy and pelvic magnetic resonance (MR) two weeks after his discharge. The perforation side was totally closed and pelvic abscess was completely resolved (Figure 2). Upon these findings, his colostomy was closed after one week. After six months of follow-up, the patient remains free from complications and sequelae. *No other pics available.  ·  · 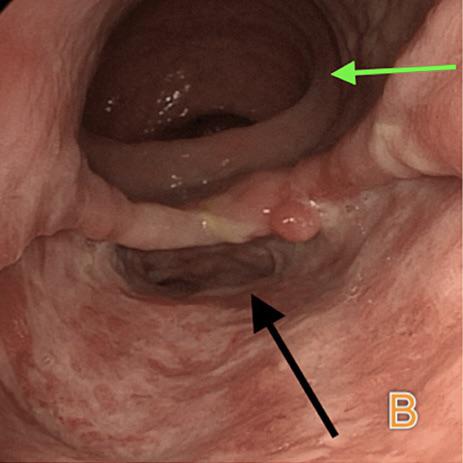 · |
|
#2
●
03-15-2023, 09:38 PM
| ||||||||
| ♚ Legacy Gold Member ♚ Poster Rank:202 Iceman Join Date: Aug 2017 Posts: 7,505 Mentioned: 19 Post(s) Quoted: 3630 Post(s)
| ||||||||
|
Re: Rectal Issues.
Rectum? Damn near killed him! Mary mary quite contrary shave that ass it's so damn hairy! So he was trying to give himself an enema and he perforated his bowel? Maybe he was enjoying it too much! "Digital examination" Doctor speak for I just shoved my finger in your bum |


















{kind=link}