|
#1
●
03-13-2023, 11:13 PM
| ||||||||
| These are the rooms Poster Rank:25 of ruin. Join Date: Sep 2014 Posts: 54,011 Mentioned: 145 Post(s) Quoted: 30403 Post(s)
| ||||||||
|
Peristomal Necrotizing Fasciitis
Source: A 24-year-old, otherwise healthy, male patient with chronic hepatitis B and a Child-Pugh Score of 5 (Class A) underwent abdominoperineal resection for stage III adenocarcinoma of the rectum at our department. He had a prolonged postoperative course due to perineal wound infection, but was finally discharged after 76 days of admission and referred for adjuvant chemotherapy. The patient presented on the day of his fourth cycle of chemotherapy. He was on the FOLFOX-4 regimen. He had received part of his cycle earlier in the morning, which included intravenous (IV) boluses of 5-fluorouracil, oxaliplatin, and leucovorin. During this treatment, he complained of having mild discomfort and irritation in the area of his stoma. Upon removal of his stoma appliance, the oncology service noted an area of necrotic skin around his stoma. He was urgently referred back to us for management. Upon arrival, the patient was alert and oriented. He was vitally stable and not in sepsis. He complained of only mild discomfort around his stoma site for the past few days. He had been using the same stoma appliance for well over a month. As he had only minimal symptoms, he did not mention these symptoms at initial presentation to the oncology service. His systemic examination was unremarkable. On examination of his abdomen, a wide area of necrotic skin and subcutaneous fat was seen extending around his end-sigmoid colostomy up to his umbilicus superomedially. The colon at the stoma site was thickened and inflamed (Figure 1). Close clinical examination revealed that the colon at the stoma site adhered very well to his abdominal wall with no dehiscence despite the overlying findings and that the necrosis had not spread beyond the deep fascia to involve the abdominal wall musculature. The rest of his abdominal examination was unremarkable, with a well-healed midline laparotomy scar of his previous surgery. The patient’s baseline labs were normal, including his total leucocyte count. As debridement was necessary and chemotherapy-induced neutropenia was anticipated after a few days, a carefully planned surgical approach was used to lessen the chances of complications during the neutropenia phase. The patient was given general anesthesia and a loop transverse colostomy was first constructed in the right hypochondrium after pulling the transverse colon through a small incision. Following this, debridement of the area of necrosis was undertaken down to the musculature, leaving an erythematous outer edge. The end-sigmoid colostomy was not taken down and its opening was closed. The two steps of using a small incision in the right hypochondrium to create the transverse colostomy rather than a midline incision and closing the end-sigmoid colostomy opening without taking the stoma down were done to avoid extra incisions and prevent even the least contamination of the peritoneal cavity. Such contamination could have occurred from the infected area (area of peristomal NF) or from colonic contents that could be spilled into the midline wound or peritoneal cavity during the dissection and mobilization of the colon. The thought process behind this approach was as follows: While deep surgical site infection and wound infection related to such contamination may not have severe consequences at the time of surgery, as the patient was immunocompetent, the chances of flare up and resultant sepsis a few days later during the chemotherapy-induced neutropenia phase could lead to severe complications and a fatal outcome at that point in time. As the end-sigmoid colostomy site was also thickened due to the inflammatory process, three punch biopsies were taken to rule out recurrence. These biopsies were subsequently negative for malignancy. Postoperatively, the patient was kept in the ward where he was given IV broad-spectrum antibiotics and IV anti-fungal agents with daily dressings of the debrided site. Subcutaneous filgrastim was started on the third postoperative day (pod). On the fourth pod, the previously closed end-sigmoid colostomy dehisced (Figure 2). Re-suturing was attempted but was unsuccessful due to friable tissue. As the newly constructed proximal transverse loop colostomy had started working from the second pod and the end-sigmoid colostomy discharged only mucus, it was decided to continue with daily dressings of this area. As anticipated, the patient developed grade 4 neutropenia (counts less than 500 cells/mm3) by the seventh pod. The patient had a single episode of high-grade fever during this time, however, he did not develop any other signs of sepsis. He was continued on the same regimen with strict observation and a repeat of daily routine laboratory tests. His counts gradually improved and became normal by the 12th pod. The patient underwent an exploratory laparotomy three weeks later for resection of his distal colon, including his end-sigmoid colostomy site, with the plan of making the transverse colostomy his permanent stoma. Although the initial punch biopsies were negative for malignancy, this option was selected, as a computed tomography (CT) scan performed during admission showed a thickening of the end-sigmoid colostomy with a suspicion of recurrence below the abdominal wall. Endoscopy was not planned preoperatively due to the risk of perforation at the friable end-sigmoid colostomy site. The patient also had a FibroScan (Echosens, Paris, France) prior to the procedure due to a history of chronic hepatitis B. This showed a Metavir score of 4.9 that was consistent with the F0-F1 stage of fibrosis. Postoperatively, the patient remained well. He was discharged on the 10th pod of his second surgery and urgently referred for completion of his adjuvant chemotherapy. Histopathology of the resected specimen did not reveal any recurrence of his cancer. The patient followed up four months later with his wound completely healed (Figure 3). 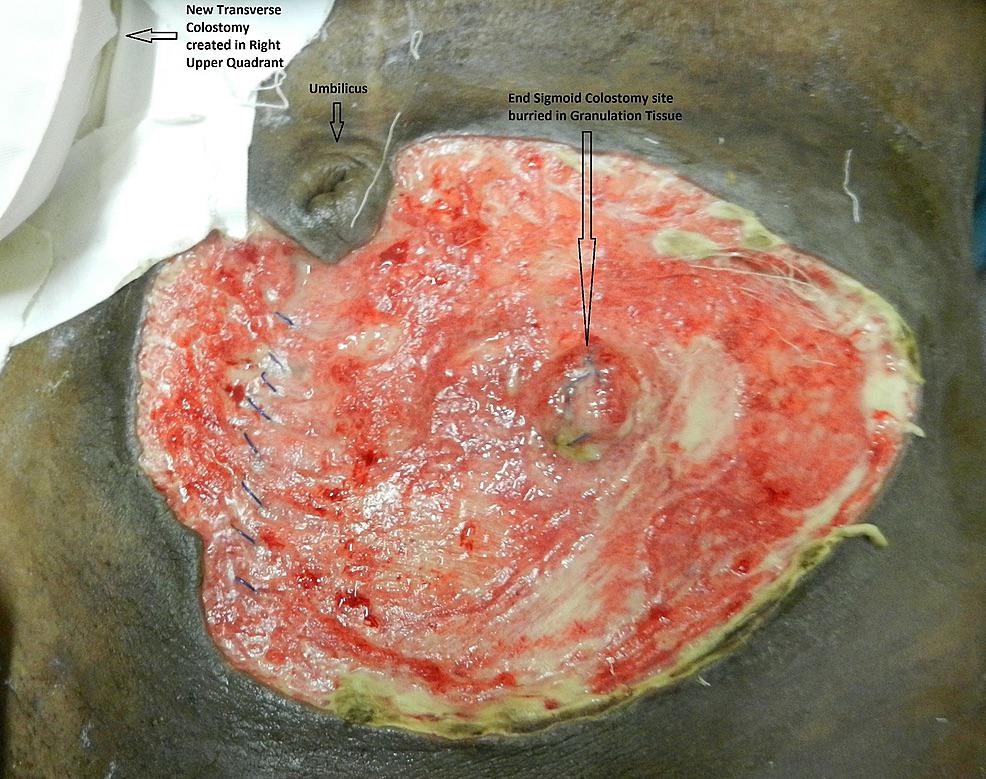 · 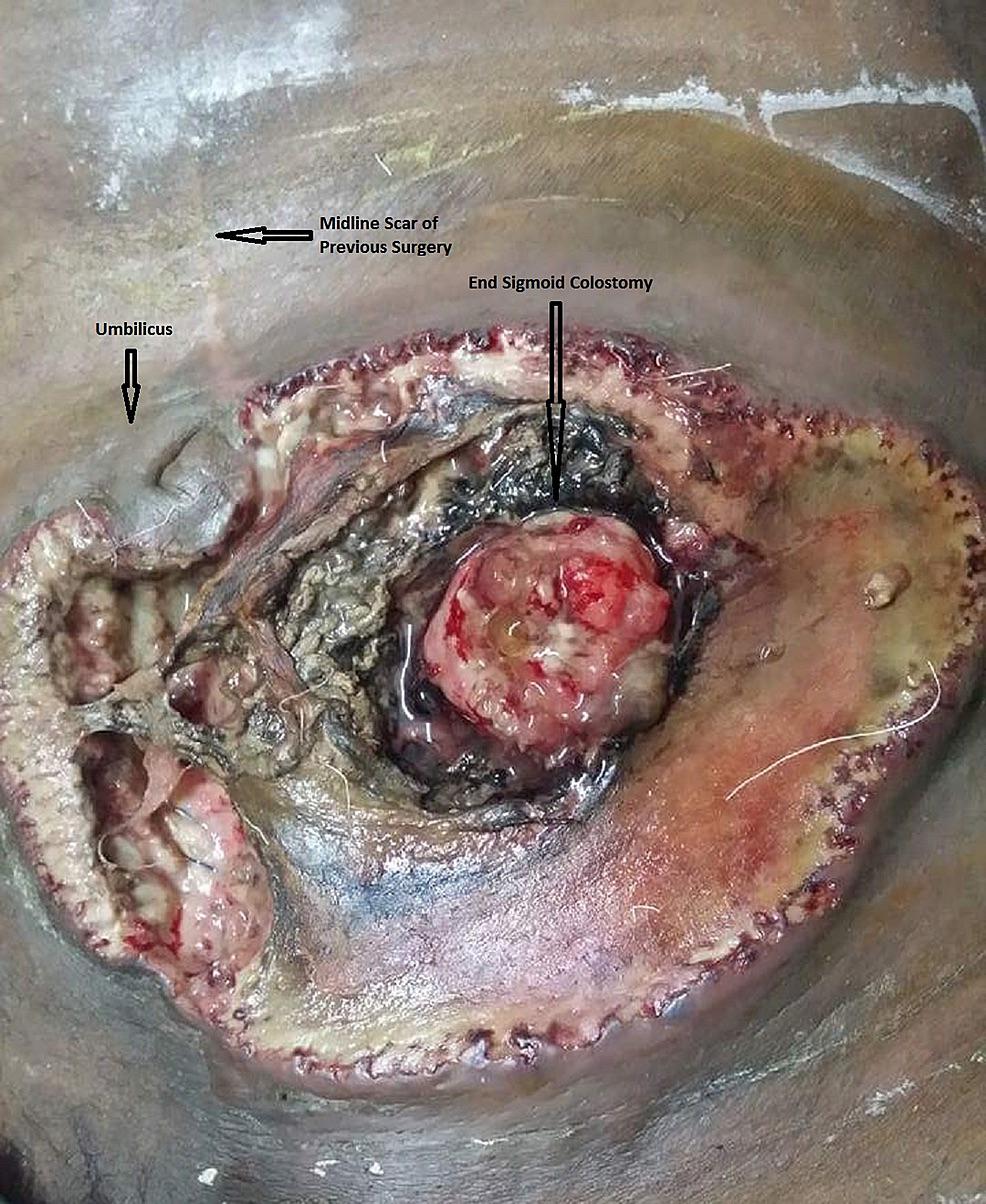 ·  · |













{kind=link}