|
#1
●
05-13-2024, 03:14 PM
| ||||||||
| These are the rooms Poster Rank:25 of ruin. Join Date: Sep 2014 Posts: 54,011 Mentioned: 145 Post(s) Quoted: 30403 Post(s)
| ||||||||
|
Necrotizing Fasciitis
>>A 23-year-old female presented to the Emergency Department (ED) of a tertiary hospital with a 12-h history of a painful and swollen right breast. The breast was entirely discoloured and an offensive nipple discharge was noted. This occurred in the context of a 3-day history of breast pruritus near the inframammary fold. The patient also complained of dizziness, nausea, and several episodes of vomiting, and denied any history of trauma to the breast. Her medical history includes obesity (BMI 34.7) and polycystic ovarian syndrome. She is not on any regular medications, is a non-smoker and drinks small amounts of alcohol socially. >>On presentation, the patient was alert and oriented, with a blood pressure of 80/60 mmHg, heart rate of 130 beats/min and saturations of 95% on room air. Her temperature was 35.8 °C. Breast examination revealed a grossly swollen and markedly tender right breast with discolouration and erythema to the margins, along with associated bullae. Examination of the left breast was unremarkable. >>Blood tests were consistent with severe sepsis with end organ dysfunction. Her initial laboratory results revealed a white cell count of 27.85 × 109/L with neutrophilia (23.6 × 109/L) and a C-reactive protein of 400 mg/L. An arterial blood gas identified a metabolic acidosis with pH of 7.06 and lactate of 8.8 mmol/L. Creatinine was elevated at 394 umol/L, with an estimated glomerular filtration rate of 13 mL/min.1.73 m2. Her international normalised ratio was 1.8 and activated partial thromboplastin time 44 s. >>Over the next few hours, the patient received 5 L of intravenous crystalloid resuscitation along with inotropic support, including boluses of metaraminol (2 mg total) and adrenaline (1.1 mg total). She remained anuric during this time. A noradrenaline infusion was commenced in ED via a central line, with a peak pre-operative rate of 1.5 mg/h. With advice from ICU, a vasopressin infusion was also commenced at 4 units/h. In light of a reported possible penicillin allergy, renal-adjusted doses of IV meropenem, IV clindamycin and IV vancomycin were administered after consultation with the infection control team. The patient was taken to the operating theatre within 3 h of her presentation and underwent an emergency right mastectomy and debridement of all necrotic tissue including pectoralis major fascia, preserving pectoralis major. A haematologist was consulted with regard to the patient’s coagulopathy and 2 units of fresh frozen plasma were administered intraoperatively to prevent excessive haemorrhage. The wound was packed and covered with a vacuum assisted closure (VAC) dressing, and the patient was transferred to the intensive care unit for post-operative care where she remained intubated and sedated. Continuous renal replacement therapy (CRRT) was commenced Fig. 1, Fig. 2, Fig. 3, Fig. 4, Fig. 5 . >>Overnight however, the patient developed a troponin-I rise to 20,203 ng/L with ST elevation in inferior leads. Troponin-I ultimately peaked at >40,000 ng/L. Adrenaline and vasopressin were gradually weaned and 2 units of packed cells were transfused in light of a haemoglobin of 83 g/L. Although likely sepsis driven myocardial ischaemia, aspirin and an IV heparin infusion were commenced following consultation by a cardiologist. >>The noradrenaline infusion rate peaked at 3 mg/hour in ICU and was weaned from 6 h post-operatively, with ultimate cessation on day 2 post-op. CRRT was ceased after 12 h in view of improving urine output and renal function. The patient was eventually extubated on day 8 of her admission, following 3 further wound debridements and VAC applications on days 1 and 5, and 9. Tissue culture returned a positive result for streptococcus pyogenes. On day 5, the patient was confirmed to have no allergies, and antibiotic therapy was changed to benzylpenicillin. Inflammatory markers gradually improved, and on day 5 she was afebrile. She was eventually stepped down to oral amoxicillin for a total of 19 days as per recommendations made by the infection control team. >>Repeat electrocardiograms demonstrated resolving ST elevation, and a transthoracic echocardiogram revealed an ejection fraction of 55% with normal systolic function, a small sized septal and inferior wall motion abnormality with mild hypokinesis of segments. Follow up CT coronary angiograms are due to be completed as an outpatient. The patient remained in ICU for a total of 12 days until she was deemed safe to go to the ward. On day 16 of her admission, the patient was transferred to a tertiary hospital with a plastic surgery service for further debridement and skin grafting of her wound from her left thigh. By this time, all blood parameters had normalised. The patient remained stable for the duration of her admission under the plastics team, and was ultimately discharged home. 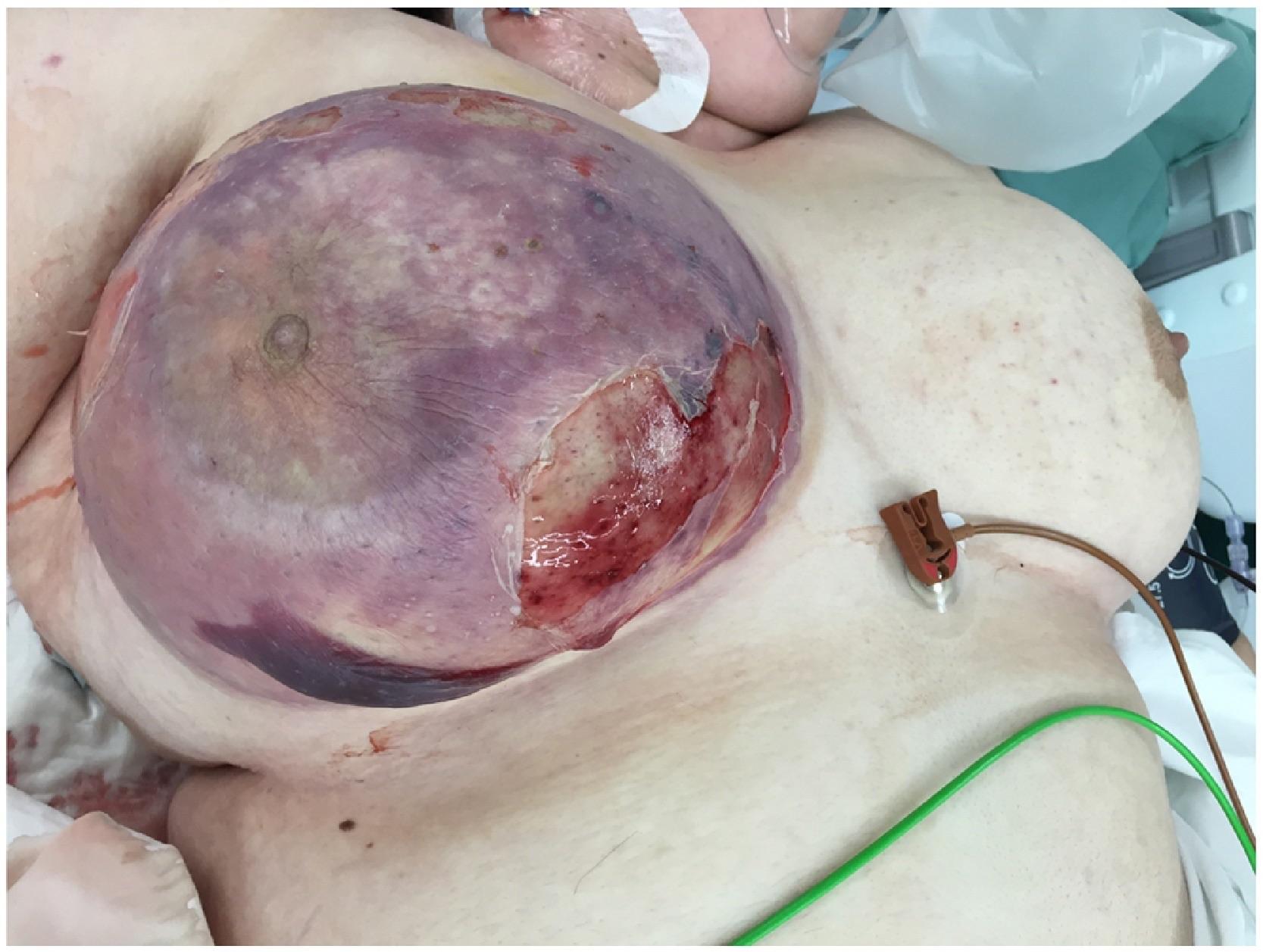 ·  ·  ·  ·  · |
|
#4
●
05-14-2024, 06:06 PM
| ||||||||
| ♚ Legacy Gold Member ♚ Poster Rank:202 Iceman Join Date: Aug 2017 Posts: 7,505 Mentioned: 19 Post(s) Quoted: 3629 Post(s)
| ||||||||
|
Re: Necrotizing Fasciitis
So remember ladies you got to wash that cheese out from under your boobies especially you big girls. Nobody likes fromunda cheese.
|
|
#5
●
05-14-2024, 06:42 PM
| ||||||||
| ☆☆☆Jumbo Lesbian Cunt☆☆☆ Poster Rank:56 My pronouns are thin/skinny Join Date: Nov 2012 Posts: 25,925
Contributions: 1
Mentioned: 160 Post(s) Quoted: 13914 Post(s)
| ||||||||
|
Re: Necrotizing Fasciitis
That areola and nipple were green. Green! A disgusting, smelly, hideously painful mass. I can't imagine having a finger rot and morph into sepsis let alone my entire boob. Damn. Nothing to do with hygiene. A scratch or puncture wound got infected. |
|
#6
●
05-14-2024, 06:53 PM
| ||||||||
| ♚ Legacy Gold Member ♚ Poster Rank:202 Iceman Join Date: Aug 2017 Posts: 7,505 Mentioned: 19 Post(s) Quoted: 3629 Post(s)
| ||||||||
|
Re: Necrotizing Fasciitis
Maybe. You know a good way to prevent infection from a scratch or puncture wound? Wash! |
|
#7
●
05-16-2024, 09:50 AM
| ||||||||
| ur gay Poster Rank:18 Join Date: Nov 2014 Posts: 60,952 Mentioned: 169 Post(s) Quoted: 36922 Post(s)
| ||||||||
|
Re: Necrotizing Fasciitis
I'm going to smack you with my unwashed titties.
|
|
#10
●
05-20-2024, 03:30 AM
| ||||||||
| My Rank: SERGEANT Poster Rank:932 Join Date: Nov 2015 Posts: 787 Mentioned: 1 Post(s) Quoted: 324 Post(s)
| ||||||||
|
Re: Necrotizing Fasciitis
I can’t believe her C-reactive protein was only 400 with a boob like that |


























