|
#1
●
07-23-2024, 06:45 PM
| ||||||||
| These are the rooms Poster Rank:25 of ruin. Join Date: Sep 2014 Posts: 54,011 Mentioned: 145 Post(s) Quoted: 30403 Post(s)
| ||||||||
|
Nasty Degloving Accident
A 36-year-old woman with no prior medical history experienced an open degloving injury to the right leg and thigh, as well as an open fracture on the lateral side of the knee, after being hit by a bus. Advanced Trauma Life Support guidelines [5] were applied to stabilize patient conditions. The injury resulted in bone loss in the distal lateral femur condyle, lateral patellar face, and lateral tibial plateau, leaving the articular surface exposed. No other injuries were present (figure 1 and 2). The patient was immediately treated according to open fracture protocol, and the plastic surgery team was called in. Emergent surgery was performed to remove the damaged skin and assess its viability for use as an autograft. Suitable skin was defatted to create a full thickness skin graft (figure 3). An extended tight, leg and knee joint debridement was performed removing non-viable tissues, including part of the lateral and posterior thigh muscles. A gastrocnemius flap was carried out to cover the lateral articular surface since there was no suitable coverage (figure 4), leaving a drainage. The defatted skin graft from the same leg injury was reattached. Stab wounds were made to drain seroma and haematoma from the recipient bed. An external fixator was performed to bridge the knee and stabilize the open fractures (figure 5). A negative pressure system, ranging from 80-100 mmHg pressure, was then applied to promote skin grafting (figure 6). The patient was prescribed prophylactic antibiotic therapy upon arrival, which included an initial intravenous dose of 1.5 grams of cefuroxime. This was followed by a repeat dose of 1 gram every 8 hours for three days, in addition to a daily dose of 250 milligrams of gentamicin for three days. After one week of admission, no signs of infection were present. The patient underwent secondary surgery to remove small areas of necrotic skin and perform a conventional skin autograft from the non-injured leg. The external fixator was removed after knee stability was assessed. The patient was allowed to perform free, controlled, and progressive knee flexion after two weeks of accident. Progressive rehabilitation therapy was prescribed and currently she achieved a range of movement 0/120º. The aesthetic result after 1 year follow-up is shown in figure 6-7. 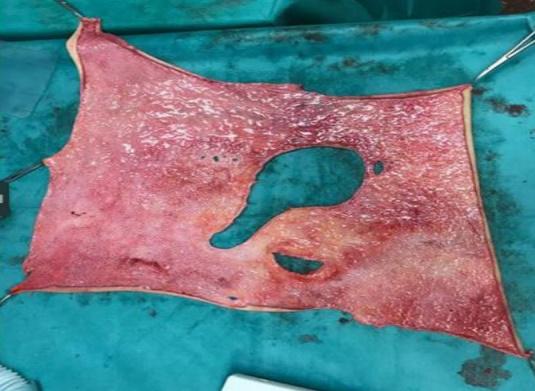 ·  ·  ·  ·  ·  ·  · |



















