|
#1
●
01-17-2023, 12:34 AM
| ||||||||
| These are the rooms Poster Rank:25 of ruin. Join Date: Sep 2014 Posts: 54,011 Mentioned: 145 Post(s) Quoted: 30403 Post(s)
| ||||||||
|
How Many Durian Fruits Mangle People a Year?
A 54-year-old male was brought to the emergency department for a sudden loss of vision in the right eye after being hit by a durian fruit. The incident occurred while he was walking under a durian tree at the back of his house. All of a sudden, a big size durian fruit (about 3 kg) fell from a tree that is about 12 feet tall. The fruit hit his right face and eye. He experienced a transient loss of consciousness for about five minutes. Subsequently, he noticed that his right vision was poor. He was not wearing any head or eye protection. He was brought immediately by his family to the hospital. On examination, there were multiple puncture abrasions over the right cheek and forehead. He also sustained a right upper lid laceration. The visual acuity in the right eye was light perception (LP) with a positive afferent pupillary defect, while the left visual acuity was 6/6. There were multiple corneoscleral lacerations with total hyphema (Figure 1). No iris prolapse or iris details was seen. There was no fundal view in the right eye. The right eyeball was soft. The left anterior segment was normal with a normal fundus appearance. The patient was diagnosed to have an open globe injury in the right eye. Urgent computed tomography (CT) scan demonstrated a “flat tire sign,” indicating globe rupture with posteriorly dislocated lens (Figure 2). The skull and orbital wall were intact with no fracture seen. There was no intracranial bleed. The patient was planned for an emergency operation under general anesthesia. A 360-degree conjunctival exploration was performed. There was a small piece of thorn measuring 3 mm embedded in the conjunctiva that was removed. The corneal and scleral wounds were sutured. Anterior chamber washout was performed. The details of the ocular injuries are shown in the diagram in Figure 3. Upper lid laceration was sutured in layers. Image post repair is shown in Figure 4. Intravitreal vancomycin and ceftazidime were administered. On further exploration, there was no visible scleral laceration up to the equator of the eyeball. The patient was started on systemic ciprofloxacin for a total duration of two weeks along with topical moxifloxacin and prednisolone acetate. There were no signs of infections that developed postoperatively with the medications. Postoperatively, his visual acuity remained LP. The patient developed recurrent episodes of hyphema. The eyeball was firm with intraocular pressure of 16 mmHg. Ultrasound B-scan revealed a total retinal detachment with extensive vitreous hemorrhage. The prognosis of the affected eye was discussed with the patient. He was also warned regarding complications of sympathetic ophthalmia. However, he was not keen on further intervention. On follow-up at one month, his visual acuity remained LP. The right anterior chamber was quiet with the presence of iridodialysis. There was no hyphema, and the intraocular pressure was 11 mmHg. The visual acuity in the right eye was persistently poor after six months of follow-up. Ultrasound B-scan showed fibrovascular traction that developed over the retinal detachment. There was no vitreous hemorrhage.  ·  · 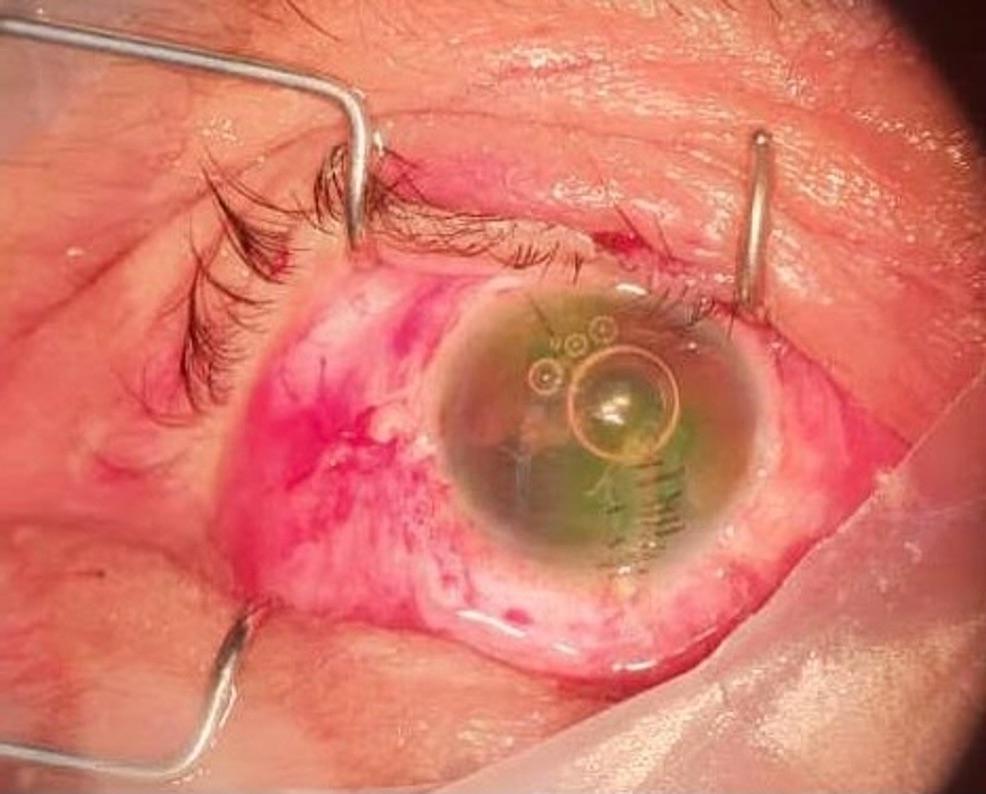 ·  · |
|
#2
●
01-17-2023, 01:43 AM
| ||||||||
| ★ Legacy Member ★ Poster Rank:248 So many choices now Join Date: Jul 2015 Posts: 5,548 Mentioned: 15 Post(s) Quoted: 2120 Post(s)
| ||||||||
|
Re: How Many Durian Fruits Mangle People a Year?
Must be overseas. I don’t even think durian are allowed in many U.S. states.
|
|
#5
●
01-17-2023, 02:41 AM
| ||||||||
| These are the rooms Poster Rank:25 of ruin. Join Date: Sep 2014 Posts: 54,011 Mentioned: 145 Post(s) Quoted: 30403 Post(s)
| ||||||||
|
Re: How Many Durian Fruits Mangle People a Year?
I just noticed it said his eyeball was soft and I wonder if that's good or bad? |
|
#6
●
01-17-2023, 06:11 AM
| ||||||||
| My Rank: MAJOR Poster Rank:93 Male Join Date: Aug 2009 Posts: 16,973 Mentioned: 9 Post(s) Quoted: 1891 Post(s)
| ||||||||
|
Re: How Many Durian Fruits Mangle People a Year?
Not surprised, they're very dangerous if falling or thrown. They taste okay but smell terrible. I actually found some here in California years ago.
|

























{kind=link}