|
#1
●
06-22-2024, 06:03 PM
| ||||||||
| These are the rooms Poster Rank:25 of ruin. Join Date: Sep 2014 Posts: 54,011 Mentioned: 145 Post(s) Quoted: 30403 Post(s)
| ||||||||
|
Hemicorporectomy
The hemicorporectomy in the reported case was performed at the Cancer Institute of the State of São Paulo in 2016. A one-stage procedure with a combined approach for closure of the vascular structures and spine was chosen and a partial-thickness flap of the left thigh was used to close the trunk in a 34-year-old male patient diagnosed with squamous cell carcinoma in a chronic pressure ulcer (Marjolin). The patient had paraplegia due to a firearm injury 26 years prior. Since 1997, he had pressure ulcers (trochanteric, ischial, and sacral) that were difficult to treat using multiple approaches. In 2013, he underwent debridement of a right sciatic ulcer and closure with a gluteal VY thigh flap. The pathological diagnosis was well-differentiated squamous cell carcinoma with involvement at the margins. In 2013 and 2014, the patient was subjected to 3 more surgical procedures due to margin expansion, but none was sufficient for total resection of the cancer, with persistence of deep margins and encroachment on the anal margins. The patient developed a fistula and infection, requiring prolonged hospitalization for broad-spectrum antibiotic therapy, creation of a loop colostomy at the right colonic flexure, and debridement of infection in the right hip. The patient had clinical stage T4N + M0 when hemicorporectomy was chosen. The lesion was ulcerovegetative and extensive, involving the perineum, gluteal region, and right posterior thigh, with foul odor and need for antibiotic venous therapy at a day hospital (Figure 1). Hemicorporectomy with curative intent and improvement of the quality of life was chosen in a multidisciplinary meeting. The patient was prepared psychologically and showed interest in undergoing the procedure, despite its magnitude. The surgical procedure involved preliminary planning by the medical teams, opting for a one-stage procedure because the patient already had an intestinal bypass. The procedure was started with the patient in horizontal dorsal decubitus (HDD) position by the oncologic surgery team. A transverse incision was made at the level of the iliac crests, and an inventory of the abdominal cavity demonstrated paracaval, bilateral iliac, and left inguinal lymphatic involvement without clinical signs of metastatic disease. The right common iliac artery and left internal iliac artery were ligated, and blood flow was maintained through the bilateral iliac veins and left external iliac artery. The plastic surgery team was responsible for dissecting the partial-thickness flap of the left thigh. A medial and lateral incision was made throughout the length of the thigh and the two incisions were joined anteriorly at the knee level. A medial incision was made between the adductor magnus and semimembranosus muscle and a lateral incision was made in the lateral intermuscular septum of the femur. Dissection was made from the distal to the proximal region in the subperiosteal plane, and ligation of the superficial femoral vessels was made distally. The adductor muscle was sectioned proximally, and the deep femoral artery was closed after excision of the vascular branches of the thigh (Figure 2). The patient was moved to the left decubitus position and the spine surgeons sectioned the spine at L4/L5 and sutured the dural sac. The position was again changed to HDD, followed by ligation of the right and left internal common iliac veins, sectioning of the remaining paravertebral muscles, and disarticulation (Figure 3). A new distal colostomy was performed for reimplantation of the ureters and closure of the peritoneum. The flap was positioned for tissue closure, excess flap tissue was discarded, closure was performed with two Blake drains, and the incisions were sutured in planes (Figure 4). The procedure lasted 16 hours and required 9,500 mL of crystalloid, 100 mL of albumin, three units of packed red blood cells, and 2,860 mL of diuresis. At the end of surgery, the patient required noradrenaline 0.3 µg/kg/min and was transferred to the intensive care unit. The patient was extubated on the first postoperative day, an oral diet was initiated, administration of vasoactive drugs was suspended on the third postoperative day, and the patient was transferred to the ward on the fourth postoperative day. Prior to preparation of this case report, the patient had been hospitalized for 25 days in the ward, fed orally, and reported being satisfied with the surgical results. One complication was a collection of 80 mL of fluid under the surgical flap, which was drained by computed tomography-guided needle aspiration, and the remaining drains were removed. There was partial loss of continuity between the epidermis and dermis along a 6-cm suture line, but surgical intervention was not required (Figure 5). 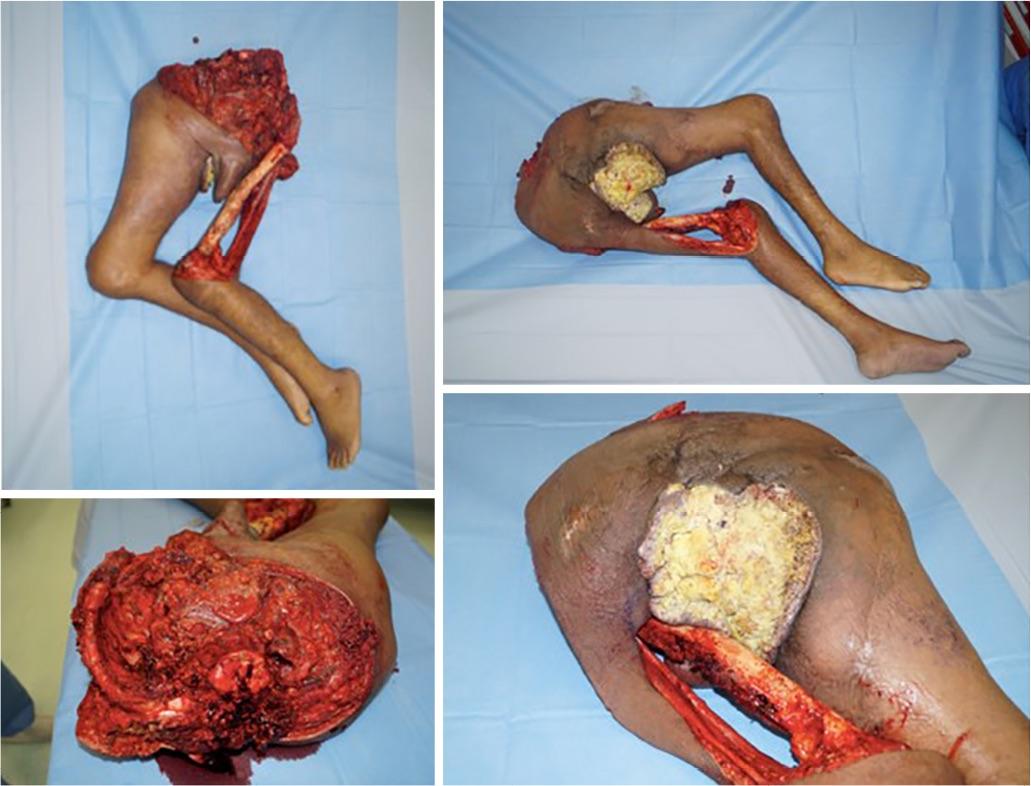 ·  ·  ·  · |
|
#3
●
06-23-2024, 04:37 AM
| ||||||||
| ★ Legacy Member ★ Poster Rank:115 Secret Agent Join Date: Dec 2009 Posts: 13,875 Mentioned: 6 Post(s) Quoted: 2901 Post(s)
| ||||||||
|
Re: Hemicorporectomy
He’s half the man he used to be. |






















{kind=link}