|
#1
●
07-22-2024, 06:20 PM
| ||||||||
| These are the rooms Poster Rank:25 of ruin. Join Date: Sep 2014 Posts: 54,011 Mentioned: 145 Post(s) Quoted: 30403 Post(s)
| ||||||||
|
Congenital Orbital Teratoma
A female baby was born at term after an uneventful pregnancy, including a prenatal ultrasound examination of the head in the 30th week which showed no anomaly. The newborn was the fourth child of non-consanguineous parents of Tunisian origin; the family history revealed no hereditary diseases. At birth, a massive protrusio bulbi on the left side was present. The ophthalmological examination showed a large protrusio and displacement of the left bulbus towards the superior nasal side (Fig. 1A). A more in depth examination was not possible even with manual eyelid opening, due to the massive displacement. The anterior part of the right eye was normal. Due to neurological monitoring of the pupil light reaction, fundoscopy could not be performed on the first day of life. The general neonatological examination revealed no other pathologic findings or tumorous disease. The MRI of the skull, performed under general anesthesia on the first day of life, showed a partly cystic, partly solid intra-orbital lesion displacing the optic nerve and the vessels to the nasal side (Fig. 2A). To relieve this extreme displacement, orbital decompression was performed by a trans-conjunctival access immediately thereafter. Eight milliliters of an amber colored liquid were punctured. After the procedure, the bulbus was moved to an origin position and the left pupil showed reaction to light exposure. Cytological, a cell population positive for the pancytokeratin marker CK22 was found, suggesting epithelial cells of unknown origin. This finding was compatible with the presence of a teratoma and made a glial lesion unlikely. The evidence of positive beta trace protein indicated parts of cerebrospinal fluid. On the 2nd day of life, fundoscopy showed a bilateral central praeocclusion with intra-retinal flame hemorrhage (Fig. 1C and D). MRI angiography excluded a cavernosus sinus venous thrombosis. After an interdisciplinary discussion with colleagues from maxillofacial surgery, pediatric neurosurgery, neonatology and pediatric oncology, a tumor resection with bulbus preservation was planned on for the third day of life. A small frontal-orbito-zygomatic approach was used to access the orbit with the aid of neuronavigation (Brianlab, Munich, Germany). After ultrasound imaging of the cyst and bulbus, the cystic sac was bluntly freed while protecting the eye muscles. To gain further access to the caudal circumference of the cyst, the sac was opened to release its tension. This allowed for complete macroscopically mobilization and enucleation of the cyst (Fig. 2, Fig. 3D). The intraoperative frozen section examination confirmed the suspicion of a mature teratoma. Due to the expansive growth of the cystic lesion, the orbital floor and lateral orbital wall were missing at the time of surgery. The eroded and enlarged orbital space and bone were reconstructed using autologous bone replacement gained from a small frontal craniotomy (10 × 20 mm) in order to avoid enophtalmos in the future (Fig. 2B). Subsequently, the frontal craniotomy bone fragment was fixed with resorbable plates and pins, the temporal muscle was refixated and the skin was closed in ordinary fashion using resorbable sutures. In the postoperative MRI, no residual tumor was seen. The infant showed a full clinical recovery, while the peri-postoperative blood loss was minimal, and no blood transfusions were needed. Lid opening was possible spontaneously, allowing occlusion therapy to be started in order to avoid amblyopia. The patient was discharged with analgesics and a topical steroid therapy, which could be stopped after 2 weeks. 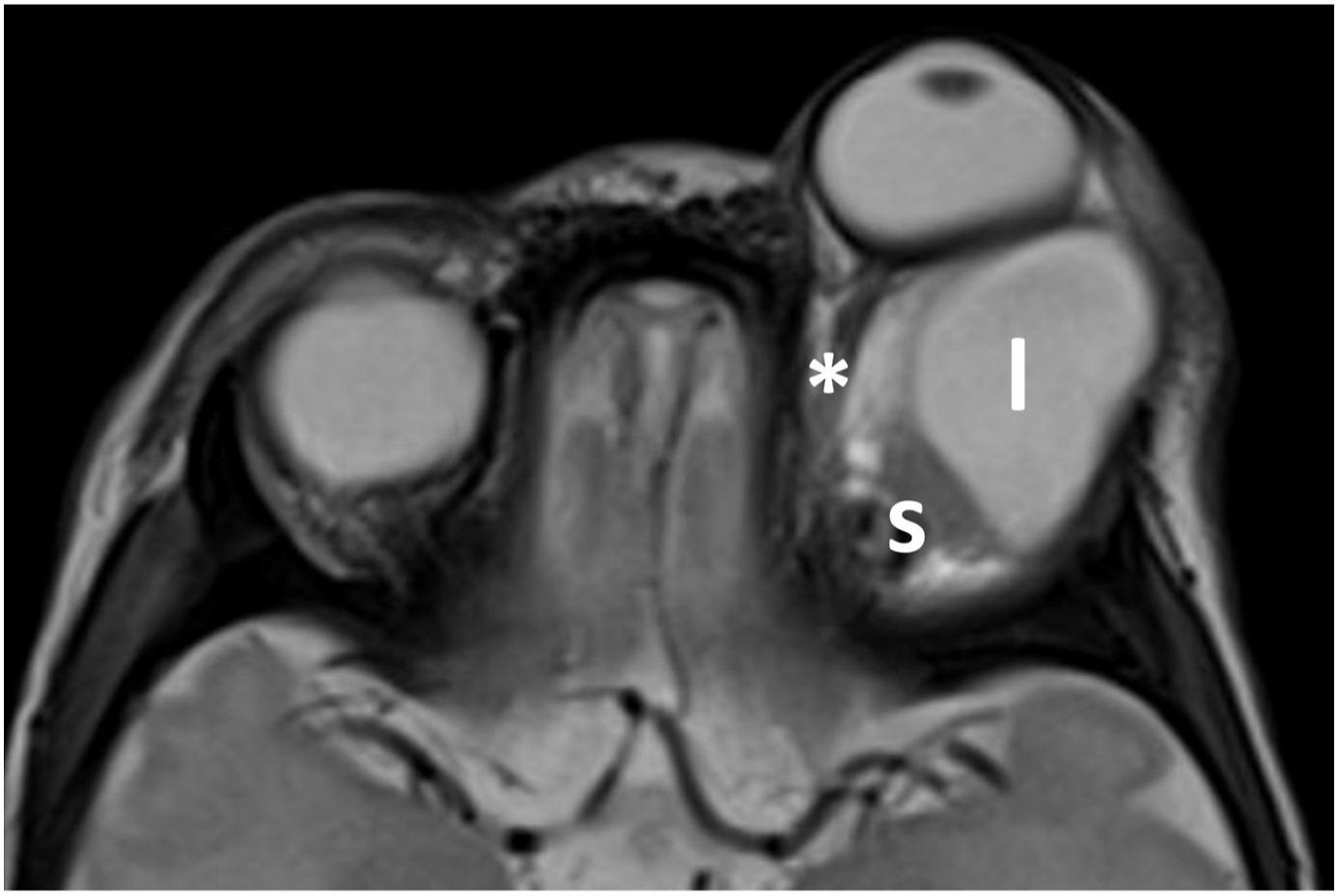 ·  · 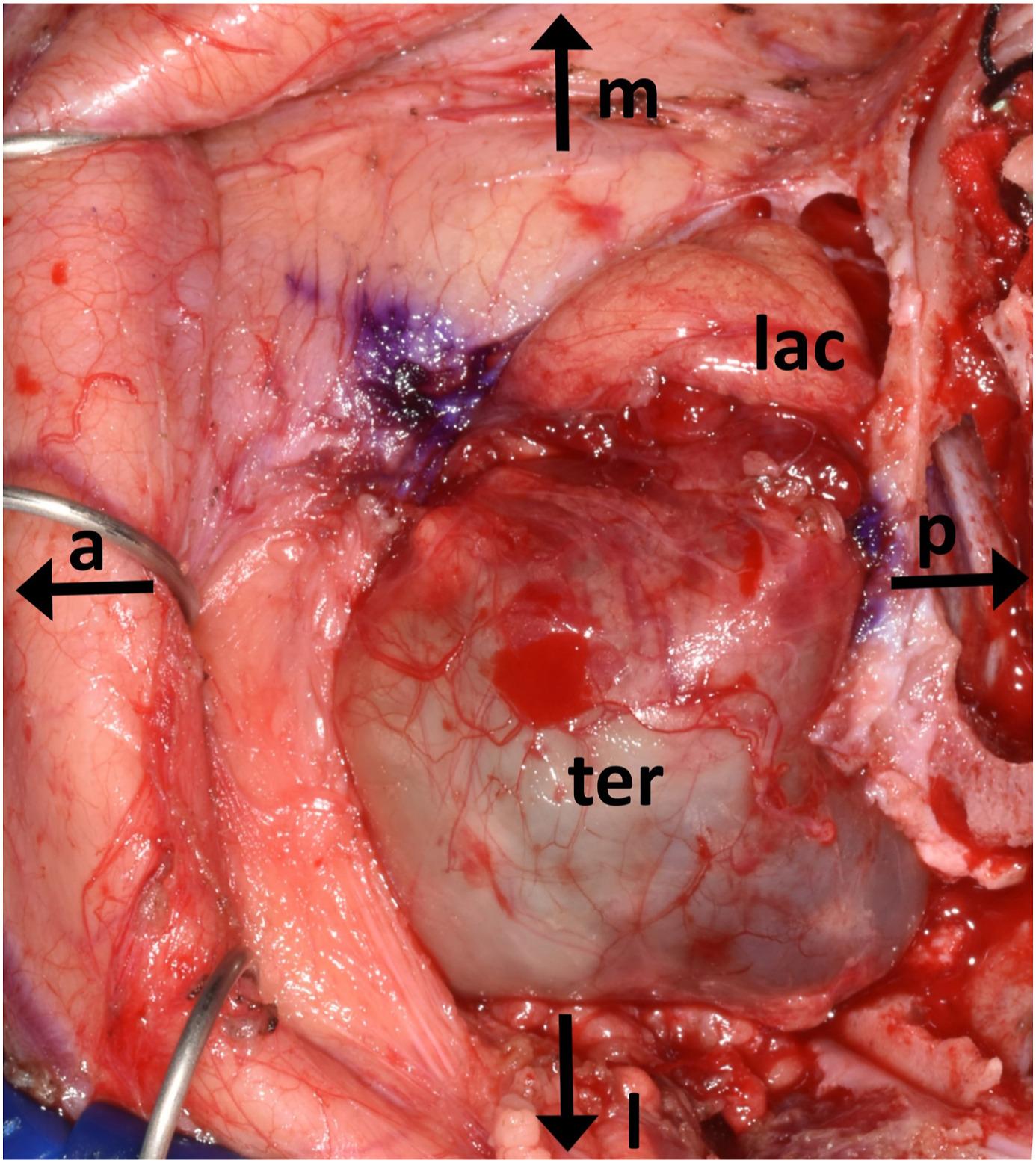 · 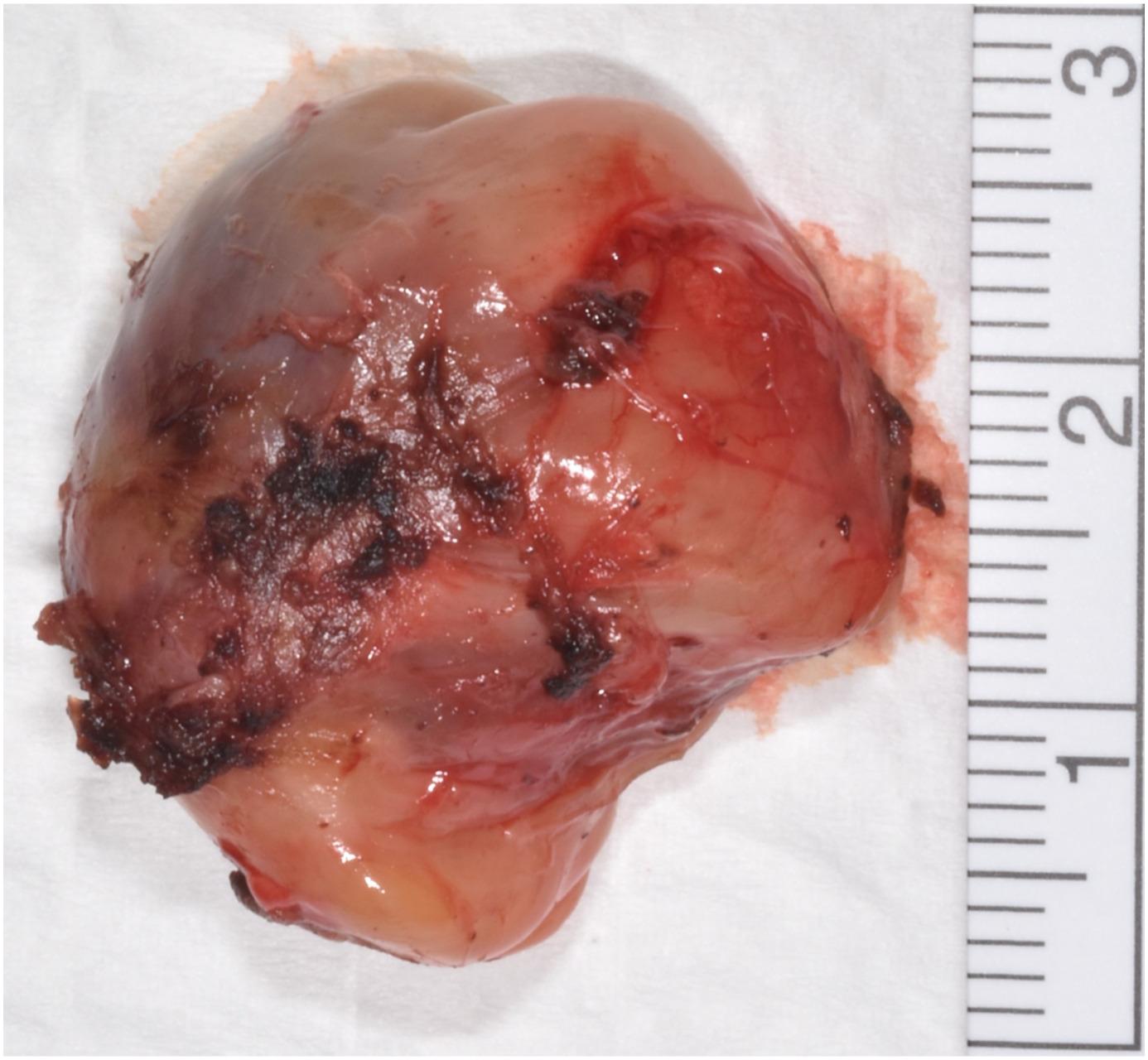 · 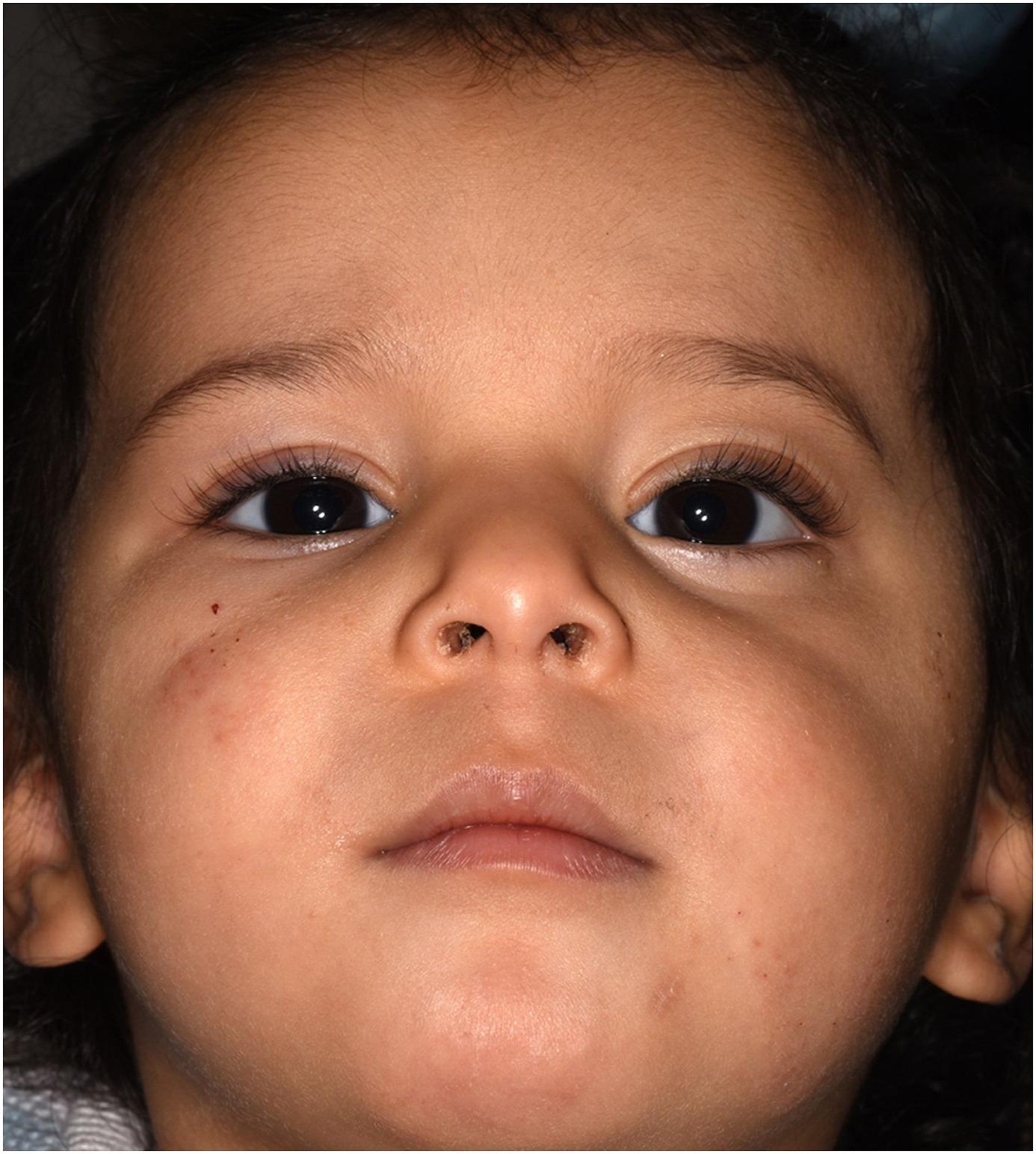 · |
|
#2
●
07-23-2024, 01:00 AM
| ||||||||
| My Rank: MASTER GUNNERY SERGEANT Poster Rank:347 Manly Man Join Date: Sep 2017 Posts: 3,601 Mentioned: 0 Post(s) Quoted: 700 Post(s)
| ||||||||
|
Re: Congenital Orbital Teratoma
Excellent recovery. |
|
#3
●
07-23-2024, 03:34 AM
| ||||||||
| ✝Mudderator from Hell✝ Poster Rank:10 e-mail Join Date: Oct 2006 Posts: 94,975
Contributions: 817
Mentioned: 472 Post(s) Quoted: 10077 Post(s)
| ||||||||
|
Re: Congenital Orbital Teratoma
props to the docs |
|
#5
●
07-23-2024, 11:56 AM
| ||||||||
| ★ Legacy Member ★ Poster Rank:119 Secret Agent Join Date: Dec 2009 Posts: 13,185 Mentioned: 6 Post(s) Quoted: 2787 Post(s)
| ||||||||
|
Re: Congenital Orbital Teratoma
Nice looking kid. Seeing those early photos I wouldn’t have expected that kind of results. I’m pleasantly surprised. |
|
#10
●
08-28-2024, 06:42 PM
| ||||||||
| My Rank: PRIVATE Poster Rank:6097 Join Date: Aug 2017 Posts: 38 Mentioned: 0 Post(s) Quoted: 3 Post(s)
| ||||||||
|
Re: Congenital Orbital Teratoma
unbelievable healing, props to the surgeons. what else is interesting is all of the intake jargon and medical terminology used in the descriptions. I'm learning a lot about medical terminology. Glad this young one did so well. |




























