|
#1
●
10-01-2024, 10:49 PM
| ||||||||
| These are the rooms Poster Rank:25 of ruin. Join Date: Sep 2014 Posts: 54,011 Mentioned: 145 Post(s) Quoted: 30403 Post(s)
| ||||||||
|
Combine Harvester Accident
: Hand wounds represent 10-15% of admissions in emergency departments in developed countries [1]. Complex lesions require urgent treatment after good clinical and radiological exams. The objective of this assessment is to adopt correct guideline for preventing functional and aesthetic sequelae. Avoiding such severe traumatisms need prevention in workplaces [2]. Surgical repair of sectioned flexor tendons has been improved in the last 40 years thanks to a better knowledge of anatomy, physiology, the development of new suture techniques and specific rehabilitation program. We report the case of a farmer admitted to emergency department at Avicenna university hospital in Rabat, Morocco, for circumferential deep wound of the right hand with exceptional laceration of the 2nd and 3rd flexor digitorum tendons from the palmar zone V. A 38 years old man, farmer, right-handed. He has sustained of a deep wound of the right hand after a work accident by the blades of a combine harvester. General exam at admission in emergency department showed stable hemodynamic status; right hand examination objectified deep, defiled, and circumferential wound interesting Zone III and the ulnar border, there was no fractures but open distal interphalangeal joint dislocation of the 5th finger; flexor tendons were intact in this zone, but abnormally wrapped; flexion of the 2nd and 3rd fingers was impossible; neuro-vascular exam showed digital hypoesthesia without pulp ischemia (Figure 1). Radiograph of the right hand showed distal interphalangeal joint dislocation of the 5th finger (Figure 2). After tetanus serum injection, the patient was transferred to the operating room, where hemostasis was addressed with electrocautery, concurrently with extensive debridement of non-viable tissue and abundant lavage with removal of foreign body (Figure 3). Both, 2nd and 3rd flexor digitorum superficialis and profundus tendons were lacerated from musculo-tendinous junction. We realized anterior approach of the distal forearm, followed by modified Kessler sutures using PDS 4.0 of the sectioned tendons (Figure 4). Curative antibiotics, local care were prescribed to its output. A dorsal hand and wrist protective splint was applied during 6 weeks, metacarpophalangeal and interphalangeal joints in flexion. On postoperative day, passive and progressive exercises for the fingers were performed; the rehabilitation process consisted of active extension and flexion during 6 weeks. After 3 month, follow-up showed interesting results; apart from keloid palmar scar and 5th finger retraction, functional hand was restored without any infection stigmata (Figure 5, Figure 6).  ·  · 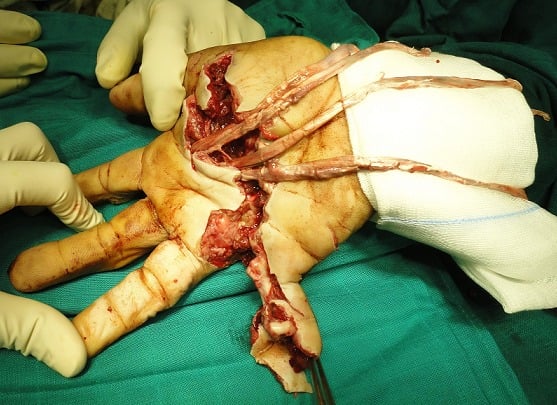 ·  ·  ·  · |
|
#2
●
10-02-2024, 11:23 PM
| ||||||||
| My Rank: MASTER GUNNERY SERGEANT Poster Rank:347 Manly Man Join Date: Sep 2017 Posts: 3,601 Mentioned: 0 Post(s) Quoted: 700 Post(s)
| ||||||||
|
Re: Combine Harvester Accident
They got that hand working good again so he could write them a check.
|















