|
#1
●
07-21-2024, 04:59 PM
| ||||||||
| These are the rooms Poster Rank:25 of ruin. Join Date: Sep 2014 Posts: 54,011 Mentioned: 145 Post(s) Quoted: 30403 Post(s)
| ||||||||
|
Car Accident
A 19-year-old woman was involved in a motor vehicle collision, and emergency medical services found her facing downward in a pool of stagnant water after ejection from the vehicle. Cardiopulmonary resuscitation was successfully performed twice in transit. Injuries included multiple spinal and extremity fractures, pulmonary contusions, a grade 2 liver laceration, intracranial hemorrhage with elevated intracranial pressures, and transient pancytopenia. The patient reached a white blood cell count nadir of 1.8 ml one day before consultation, which increased to 13.2 ml over a period of 3 days. The prealbumin level was 6.7 mg/dL and the C-reactive protein level was 371mg/L at the time of consultation. In persons aged14 to 19 years, the normal prealbumin level is 22 to45mg/dL and the normal C-reactive protein level is below 3.0 mg/dL. The patient’s glucose level ranged from 108 to 160 mg/dL; it should be noted that amphotericin B contains 900 mg of sucrose per 50 mg. Three days after admission, the oral and maxillofacial surgery service was consulted regarding progressive facial ecchymosis (Fig 1). The region was limitedto the nasolabial folds. The endotracheal tube holder was removed to prevent additional pressure on facial tissues, and the endotracheal tube was wired to the teeth. The margins of the process were marked with a surgical marker and observed hourly. A maxillofacial computed tomography scan showed evolving pansinusitis (Fig 2). The patient was empirically administered amphotericin B because of the clinical appearance and mechanism of injury in the setting of resolving pancytopenia. The infectious disease, ophthalmology, and neurosurgery departments were consulted. Within 6 hours of consultation, because of the aggressive nature of the disease process and clinical suspicion of a fungal entity, the patient underwent a biopsy of the tissue (Fig 3). A 2.5 x 0.5–cm piece of tissue from the right nasolabial fold was biopsied and submitted for tissue culture, gram stain, fungal preparation, and permanent specimen processing. Despite the initial debridement and biopsy, the infection continued to progress, and the patient was again transferred to the operating room for additional debridement and excision of necrotic tissue (Fig 4). Forty-eight hours after the initial presentation, she underwent a third operation that involved aggressive surgical debridement of infected, necrotic tissue performed in combination with aggressive increasesin amphotericin B to 5 mg/kg (Fig 5). Pathologic specimens showed Rhizopus, and cultures grew Zygomycetes species. Despite aggressive surgical and medical treatment, the patient was withdrawn from care and subsequently died of her constellation of injuries. Had she survived, maxillofacial prosthetics, multiple free flaps, or a facial transplant would have been considered as reconstructive treatment options. 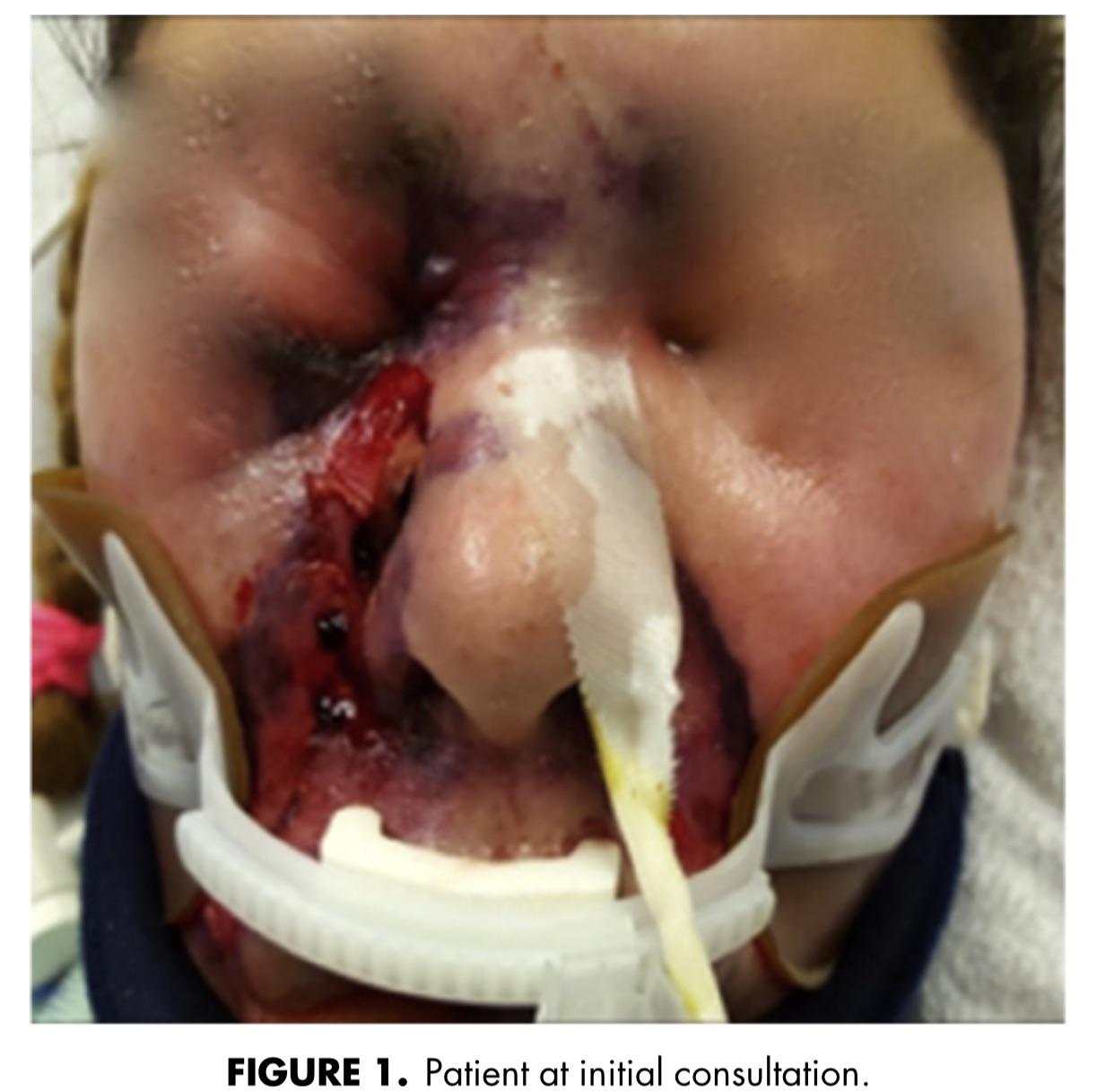 · 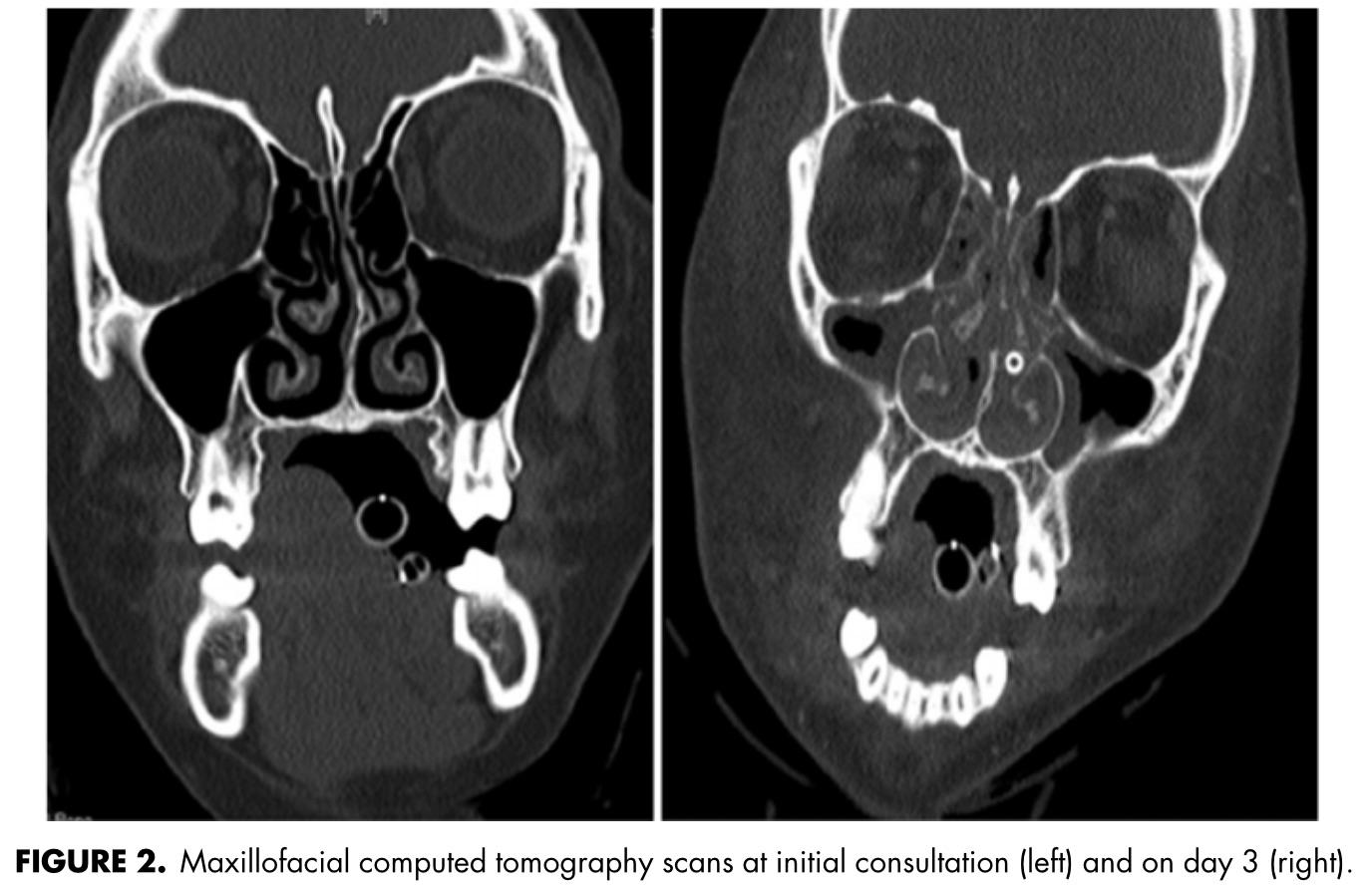 ·  ·  · 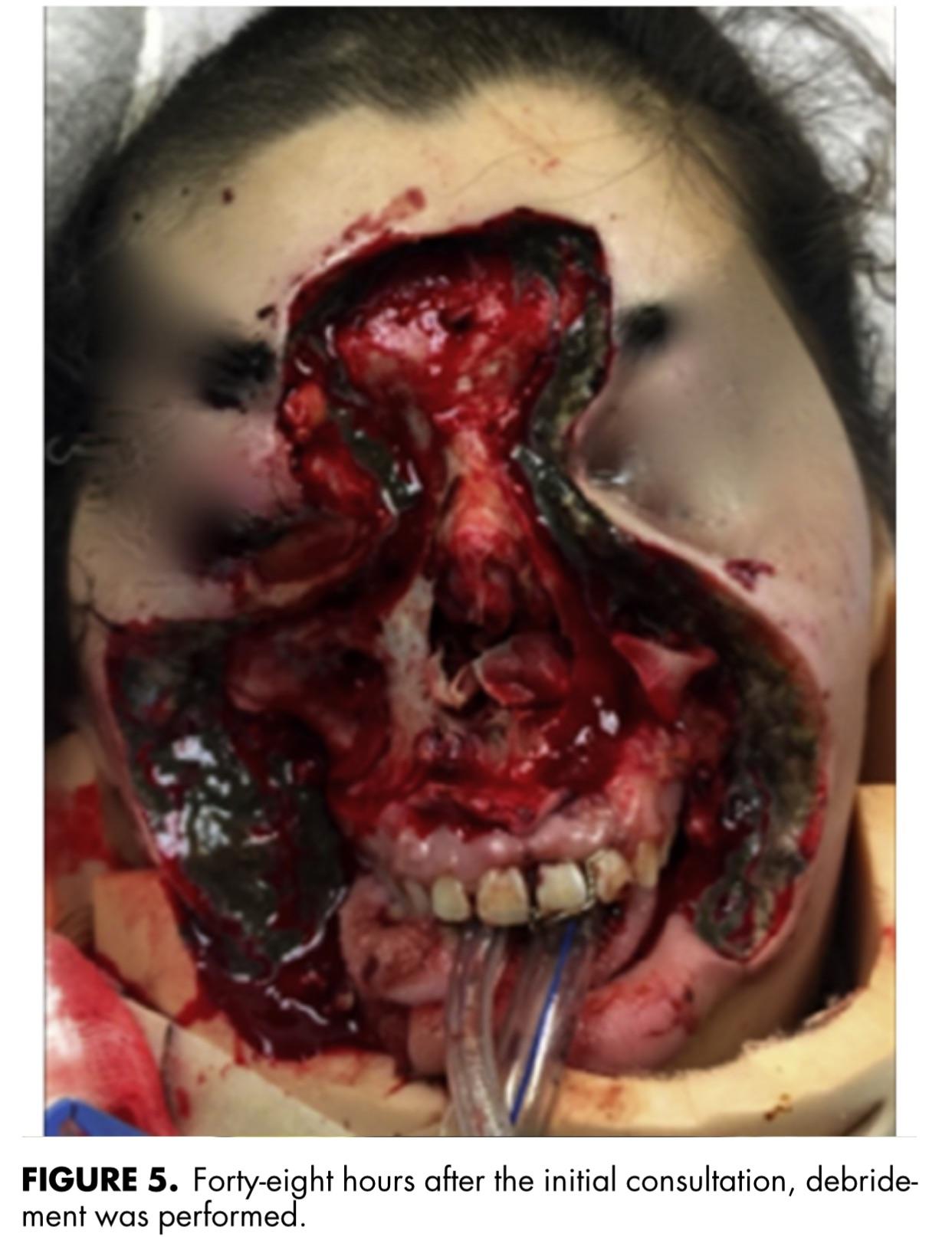 · |

























