|
#1
●
05-01-2024, 09:11 PM
| ||||||||
| These are the rooms Poster Rank:25 of ruin. Join Date: Sep 2014 Posts: 54,011 Mentioned: 145 Post(s) Quoted: 30403 Post(s)
| ||||||||
|
Bear Attack
A 55-year-old male farmer from Daporijo, Arunachal Pradesh, was referred to our hospital in September 28, 2015, with history of bear mauling. He went to the forest to hunt and tame wild bovines (Bos frontalis). He unexpectedly came across a bear (Ursus thibetanus). The bear attacked his upper body as he tried to defend himself, as a result of which, he sustained multiple soft-tissue injuries on his arms, scalp, and face. The patient was bleeding profusely and was initially admitted in the primary health-care center and stabilized, and was later referred to our hospital. >>The patient was admitted and shifted to emergency room, where the preliminary examination revealed wounds on the right side of his face and scalp as well as both forearms. He had a scalp wound in the occipital region of 10 cm × 12 cm size [Figure 1]. Facial wound approximately 15 cm long extends from the right lateral forehead to 3 cm superior from the right mandibular angle and medially across the upper and lower eyelid till the bridge of the nose [Figure 2]. His right orbital cavity was also involved in the injury, and the right orbit appeared to be avulsed. He sustained right-side partial facial nerve and maxillary nerve injury along with loss of vision. He also sustained multiple fractures of the facial bones. A preliminary examination revealed fracture of the right zygoma and right maxilla which was later confirmed by radiographic diagnostic imaging [Figures [Figures33 and and4].4]. As the bear ran away, we were uncertain of any rabies infection. Hence, antirabies vaccine was administered along with tetanus vaccine prophylactically. The wounds were debrided under local anesthesia, and any bleeding points were identified, and hemostasis was achieved; the wound was sutured with 3-0 silk sutures, and dressing was done. >>The patient was initially semiconscious, disoriented with no episodes of vomiting or bleeding through ear or nasal cavity after the incident. On admission, the Glasgow coma scale(GCS) was recorded to be 13/15. Neurosurgical consultation was sought. The neurosurgical team ruled out any intracranial lesion. After 48 h, the GCS had improved to 15/15. >>Radiographic investigations revealed fracture of right zygomatic complex, involving the frontozygomatic suture, zygomaticomaxillary suture and fracture of zygomatic arch. The infraorbital foramen and maxillary antrum were involved in the fracture line (zygomaticomaxillary), the fracture line terminated superior to the maxillary tuberosity. >>Four days after the incident, the patient was operated. The fracture was treated with open reduction and internal fixation with 1.5-mm titanium plates and screws. The zygoma was fractured from maxilla, temporal, and frontal bones into two large fragments. To align the fragments into position, two titanium screws were drilled into the fragments such that their placement does not hamper plate fixation [Figure 5]. Fragments were manipulated into anatomic location, and after plate fixation, the two screws were removed. The orbital rim was reconstructed. Fixation was initially done on the maxillary fragment and later on the zygoma. Zygomatic arch was also stabilized with 1.5-mm titanium plate and screws. Any small bony fragments were sacrificed to minimize any chance of necrosis due to loss of periosteum. Ophthalmic surgeon performed soft-tissue reconstruction of the upper and lower eyelids. Traction sutures were placed from the upper eyelid downward to improve eyelid closure postoperatively. The wound was approximated in layers with resorbable sutures [Figure 6]. >>After 2 weeks, postsurgical complication of salivary fistula was noted in the parotid region. Antisialagogues were administered, and the patient was closely observed for 2 weeks. As the result was not satisfactory, the patient had to undergo superficial parotidectomy under general anesthesia. Follow-up was done for 1 year. Facial nerve injury was noticeable in the upper eyelid region and during smiling. After 8 months, the patient showed fair amount of improvement from facial nerve paralysis [Figures [Figures77–10].  ·  · 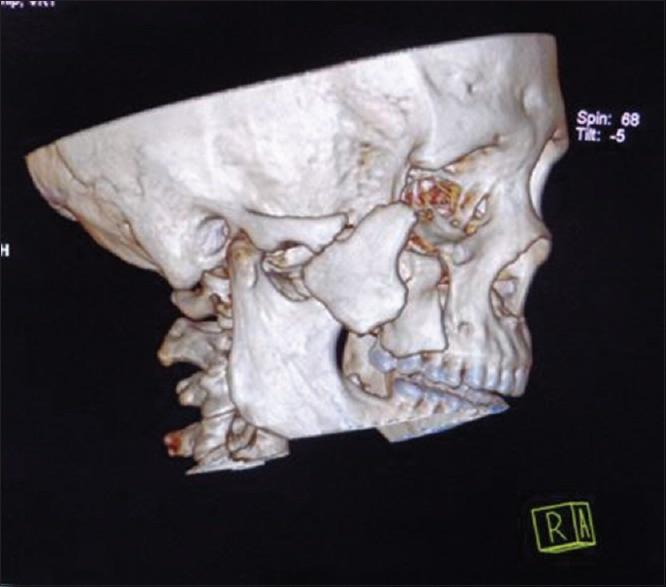 · 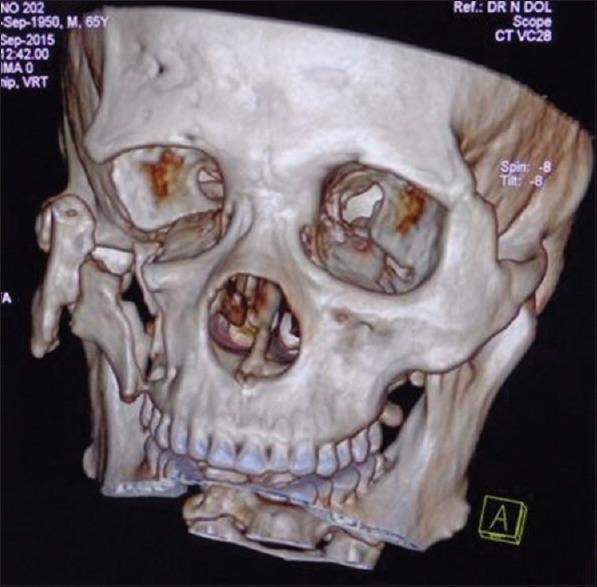 ·  ·  ·  · |
|
#2
●
05-02-2024, 01:16 AM
| ||||||||
| ★ Legacy Member ★ Poster Rank:247 So many choices now Join Date: Jul 2015 Posts: 5,548 Mentioned: 15 Post(s) Quoted: 2120 Post(s)
| ||||||||
|
Re: Bear Attack
This won’t be long, so bear with me. Eye don’t see much damage. Some mind and body healing is recommended. He should go see a local Yogi to help him with his Boo-Boo. |
|
#3
●
05-02-2024, 02:39 AM
| ||||||||
| ✝Mudderator from Hell✝ Poster Rank:10 e-mail Join Date: Oct 2006 Posts: 95,008
Contributions: 817
Mentioned: 472 Post(s) Quoted: 10082 Post(s)
| ||||||||
|
Re: Bear Attack
He should consider himself lucky as i've seen much more damage from bear attacks
|