|
#1
●
05-17-2021, 03:21 PM
| ||||||||
| ♚ Legacy Gold Member ♚ Poster Rank:907 Join Date: Jul 2020 Posts: 820
Contributions: 10
Mentioned: 13 Post(s) Quoted: 173 Post(s)
| ||||||||
|
Suicide by Bomb, with Decapitation
This has been posted here before but not with the same image quality. Mishawaka, Indiana, US. In the fall of 2011, the badly injured body of a 65-year-old male was found on its back in the backyard of his home (Figs.1-3). A suicide note was found in the home, which indicated that the decedent wanted to “take the quick way out” of life, saying that he was depressed and in pain. Investigative information confirmed that the man was a military veteran with training in explosives. The victim’s neighbors and brother, who contacted police as they had not heard from him in some time, explained that the decedent was constantly using explosives. The neighbors had mentioned that four days prior, they had heard and felt the biggest explosion they had ever heard from his property but had not contacted anyone since he was always blowing things up.  Fig.1 Scene photograph showing the victim in a collapsed lawn chair in the middle of the backyard of his rural residence, with notable absence of the head.  Fig.2 Knee injuries.  Fig.3 Absence of head and neck structures. Upon arrival at the scene and discovery of the body, police were initially concerned about additional explosive devices, as the decedent had previously expressed anti-government sentiment. This fear was heightened by the presence of a hand-held remote detonator device and another electrical device at the scene. As a result, the bomb squad was called and a robot was used to closely examine the remains and the scene prior to moving the body (Figs.4-5). There were no more explosives found near the body, but unarmed explosives were found in the decedent’s residence and disposed of at the scene. 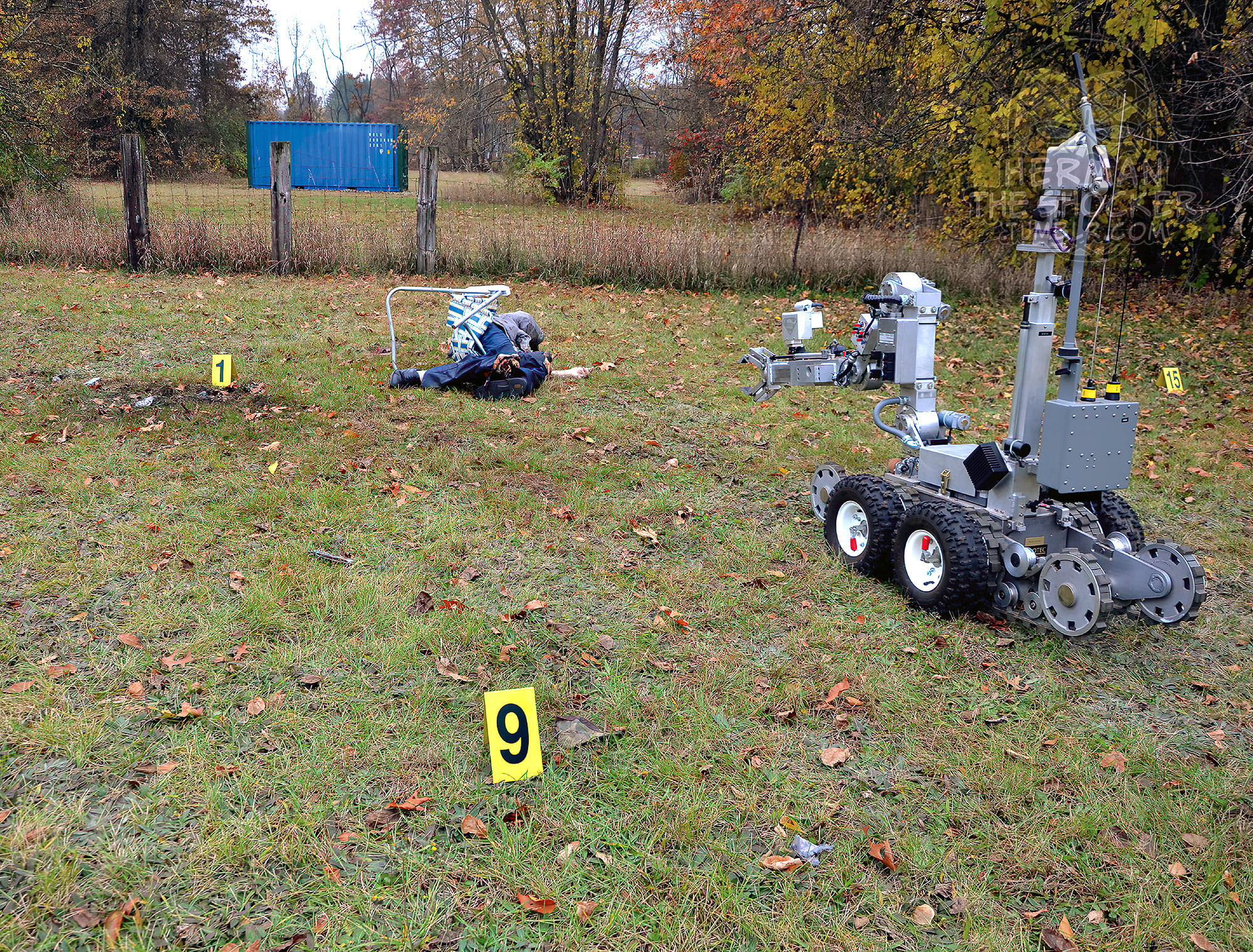 Fig.4 Bomb squad robotic device used to perform initial body exam.  Fig.5 There were no more explosives found near the body. Autopsy examination revealed a well-developed, well-nourished, male whose appearance was altered by severe injury. Radiographs revealed extensive skeletal trauma to the upper torso, with absence of head and neck structures as well as fractures about the knees. There was no radio-opaque foreign material/shrapnel evident by radiographic exam. Explosive-type defects were noted on the upper aspects of the torso clothing, as well as on the knee portions of the pants. The head and neck were absent and there was extensive damage to the upper torso (Fig.6). The anterior and posterior skin of the upper chest and shoulders demonstrated irregularly jagged borders with areas of soot and charring focally. The soft and bony tissues underlying the borders were markedly damaged by presumed explosive injuries. There were rare abrasions and contusions of the chest and upper extremities. The lower extremities demonstrated rare abrasions and contusions as well as severe lacerations of the anteromedial knees with underlying fractures of the distal aspects of the femora (Fig.7). Within the depths of the knee wounds, there was soot and charring noted.  Fig.6 Absence of head and neck, with injuries of shoulders/upper chest.  Fig.7 Knee injuries. On internal exam, portions of the heart and lungs were evident within the chest cavity but were severely pulverized due to extensive blast-type injuries; the diaphragm was lacerated bilaterally and extensive pulverization-type injuries affected the liver as well (Fig.8). The upper esophagus, aortic arch, trachea, and main-stem bronchi were absent. The descending thoracic aorta and lower esophagus demonstrated lacerations. The clavicles were not readily identified, while the sternum, both scapulae, and ribs 1 through 10 bilaterally showed numerous fractures; the vertebral column was absent above the level of thoracic vertebral body 6 (Fig.9). There was a laceration of the left flank, from which a portion of the small intestine protruded. Rare contusions of the small intestines, transverse colon, and mesentery were evident. Although there was evidence of apparent charring focally on the clothing and skin, there was no visibly identifiable foreign material evident. Swabbings of the hands and injured tissue margins were collected and retained (Fig.10). The clothing was retained as well (Fig.11). 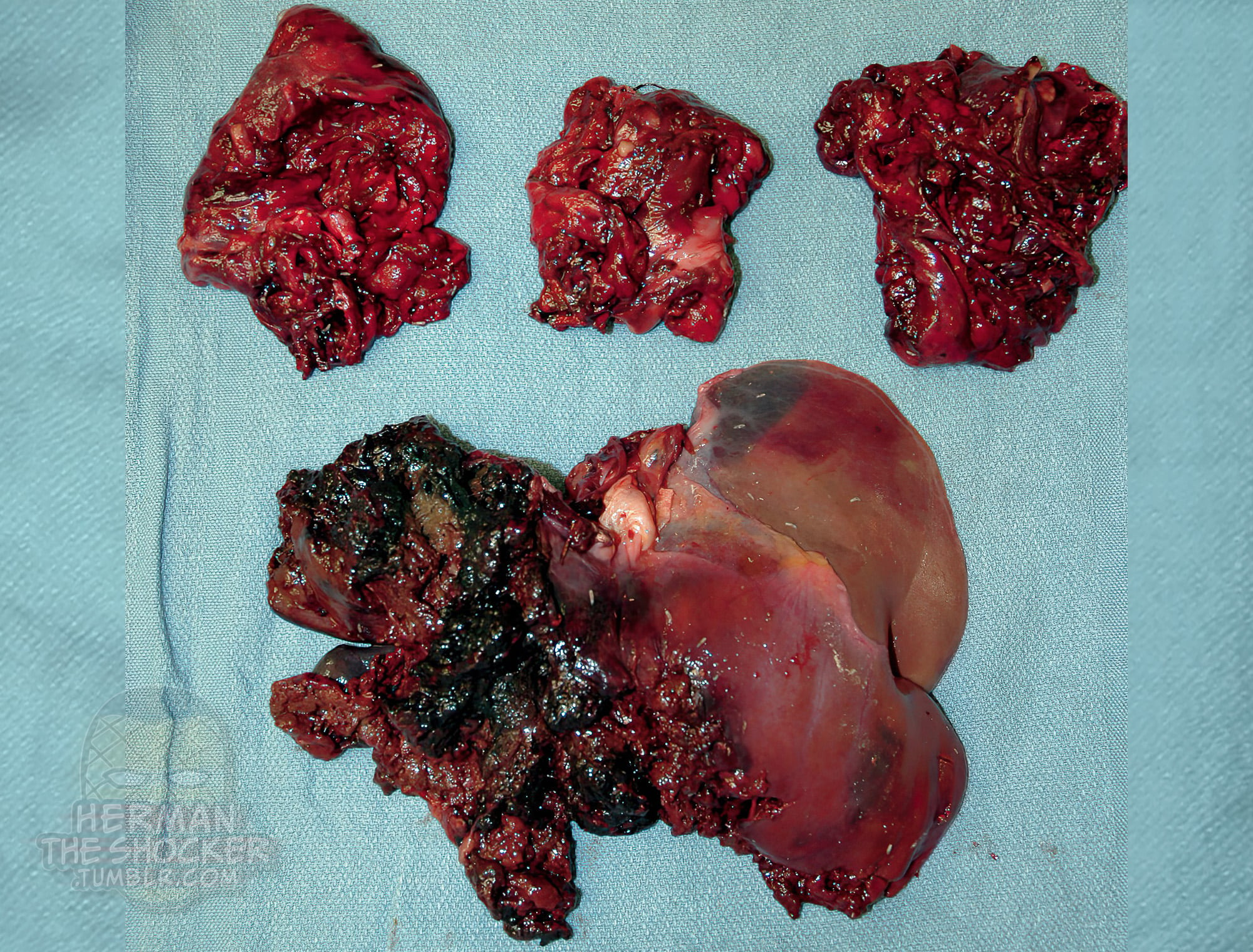 Fig.8 Irregularly ragged, badly injured remnants of both lungs and the heart (upper central) were present within the chest, and the liver showed extensive injuries as well. 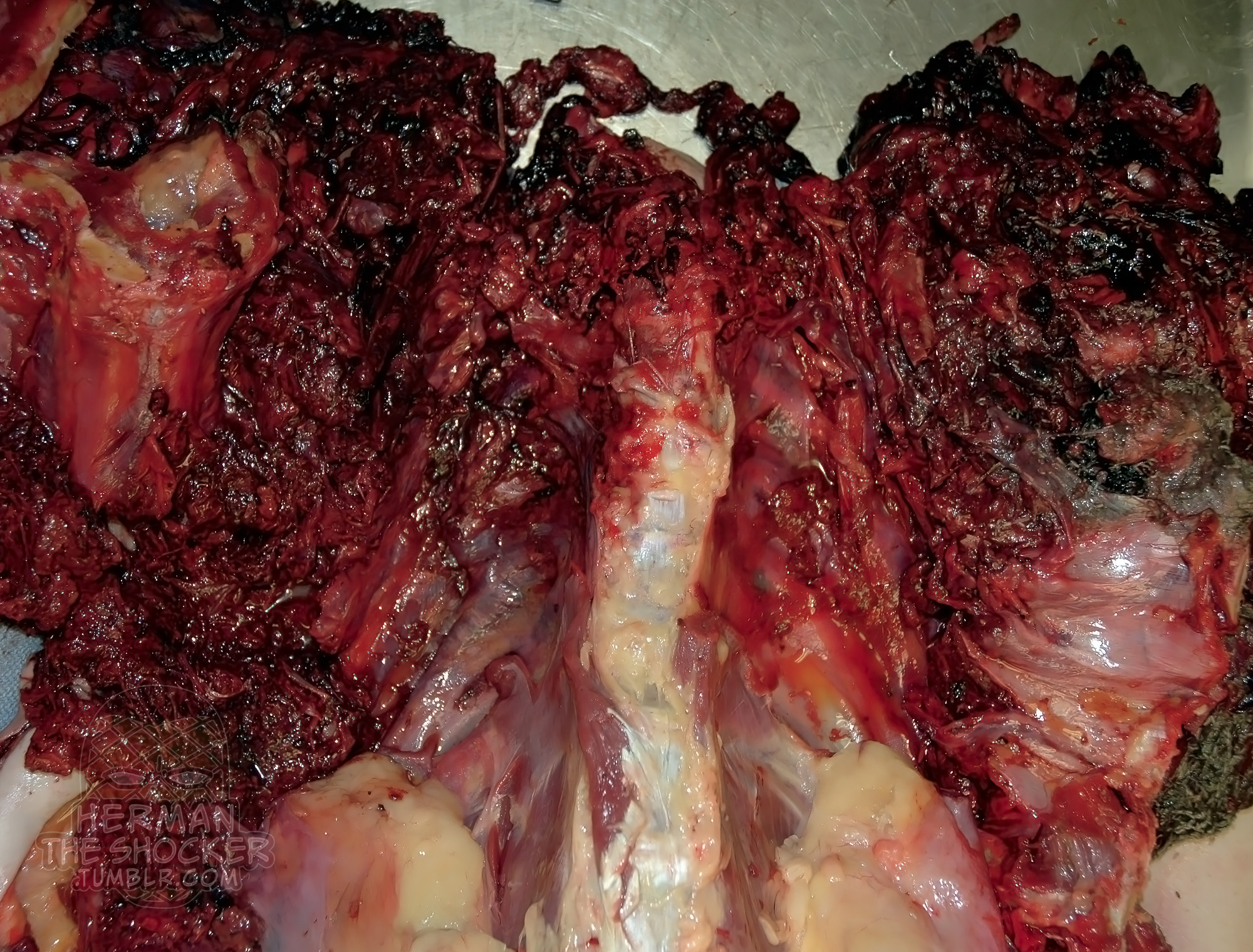 Fig.9 The appearance of the upper torso after removal of the injured internal organs, showing extensive musculoskeletal trauma. Because of the extent of injury, there was virtually no blood remaining in the body; therefore, blood toxicology testing could not be performed. A urine drug screen tested positive for opiates, acetaminophen, topiramate, norcyclobenzprine, and dihydrocodeine. The body was only tentatively identified at the time of autopsy, based on circumstance. Subsequent positive identification was made by fingerprint comparison. The cause of death was explosion/blast injuries from a bomb. The manner of death was suicide. Reconstruction of the event suggested that the decedent sat in a lawn chair, placed the explosive device between his knees, and leaned forward, with his head close to the device. The decedent had apparently purposefully kept his hands/fingers away from the explosion, apparently knowing that visual identification would be impossible after the explosion, but fingerprint comparison would be possible. As the case was deemed an obvious suicide by the coroner and police investigators, no further testing was undertaken to determine the exact nature of the explosives used in this event. As such, despite the collection of trace evidence and clothing, no further examination was performed.  Fig.10 Hand swabbings were collected in case testing for explosives was to be undertaken.  Fig.11 A photograph of the T-shirt that the decedent was wearing at the time of the explosion. Suicidal explosions are rarely encountered in the United States, although in some places worldwide, suicidal terrorist bombings are encountered to some degree of regularity, and the nonterrorist variety may be more common in other nations. Many of the reported cases of suicide by explosives report destruction of the head; however, rarely do they result in complete decapitation. While suicidal deaths related to explosives are not common, it is important that forensic pathologists and death investigators be aware of the characteristics of explosives-related deaths. - This post is for educational purposes only and is nonprofit. Under Section 107 of the US Copyright Act of 1976; Allowance is made for "Fair Use" for purposes such as criticism, comment, news reporting, teaching, scholarship, and research. OP is not a medical expert. No copyright infringement intended. This post does not encourage or glorify violence/harassment. Images might have been upscaled and enhanced. Text might have been shortened and simplified/reorganized for online view. Original case report by McLemore A.M., Prahlow S.P., Prahlow J.A. - Forensic Pathol 2016. |
|
#2
●
05-17-2021, 03:25 PM
| ||||||||
| Für Immer Verloren Poster Rank:50 Boredom + Despair Join Date: Sep 2017 Posts: 30,253
Contributions: 666
Mentioned: 136 Post(s) Quoted: 10331 Post(s)
| ||||||||
|
Re: Suicide by Bomb, with Decapitation
Excellent thread, as always, thank you.
__________________ "I'd give the world for the chance just to see your face again. Still I pretend that you're still standing by." |
|
#3
●
05-17-2021, 03:37 PM
| ||||||||
| My Rank: STAFF SERGEANT Poster Rank:851 Flesh and Blood Join Date: Apr 2012 Posts: 895 Mentioned: 3 Post(s) Quoted: 352 Post(s)
| ||||||||
|
Re: Suicide by Bomb, with Decapitation
Wow, he certainly did a number on himself. 'He liked blowing things up' said the neighbours |
|
#5
●
05-17-2021, 03:46 PM
| ||||||||
| My Rank: LANCE CORPORAL Poster Rank:3352 Join Date: Sep 2013 Posts: 108 Mentioned: 0 Post(s) Quoted: 47 Post(s)
| ||||||||
|
Re: Suicide by Bomb, with Decapitation
But what do you suppose happened to his head? Vaporized? Or is someone going to find it on their lawn or when they are clearing out their gutters?
|
|
#6
●
05-17-2021, 04:48 PM
| ||||||||
| My Rank: SERGEANT MAJOR Poster Rank:298 Join Date: Mar 2010 Posts: 4,288
Contributions: 1
Mentioned: 2 Post(s) Quoted: 1439 Post(s)
| ||||||||
|
Re: Suicide by Bomb, with Decapitation
Excellent and informative thread. Most certainly appreciate your continued posting of such material.
|
|
#9
●
05-17-2021, 08:59 PM
| ||||||||
| My Rank: FIRST SERGEANT Poster Rank:474 Male Join Date: Dec 2009 Posts: 2,258 Mentioned: 0 Post(s) Quoted: 293 Post(s)
| ||||||||
|
Re: Suicide by Bomb, with Decapitation
Have you ever wondered what the effect of explosives are on the human body? Well look no further, we got your answers right here.
|
|
#10
●
05-17-2021, 10:52 PM
| ||||||||
| ♚ Legacy Gold Member ♚ Poster Rank:99 Male Join Date: Nov 2009 Posts: 16,492 Mentioned: 6 Post(s) Quoted: 4547 Post(s)
| ||||||||
|
Re: Suicide by Bomb, with Decapitation
Kid comes up with head in his little wagon. Adults: "Oh, that's just old Ed's head! He always used to blow stuff up. Just put it right back where you got it!" |




























