|
#1
●
04-29-2013, 04:22 AM
| ||||||||
| ★ Legacy Member ★ Poster Rank:368 I need a nap =| Join Date: Aug 2012 Posts: 3,203
Contributions: 43
Mentioned: 42 Post(s) Quoted: 901 Post(s)
| ||||||||
|
What is This Nasty Shit?
Grossness  Anybody know what this is? This is far to severe to be plain ol' acne, or abscess' isn't it? |
|
#2
●
04-29-2013, 04:57 AM
| ||||||||
| My Rank: SERGEANT Poster Rank:1171 Join Date: Sep 2009 Posts: 541 Mentioned: 0 Post(s) Quoted: 50 Post(s)
| ||||||||
|
Re: What is This Nasty Shit?
Yeah it's severe alright! Looks kind of soft though, I wonder if it's filled with puss. Or then it's a good old tumor. Anyway it looks like a turtle backpack.  |
|
#3
●
04-29-2013, 05:39 AM
| ||||||||
| My Rank: FIRST SERGEANT Poster Rank:417 Male Join Date: Dec 2012 Posts: 2,771
Contributions: 30
Mentioned: 6 Post(s) Quoted: 387 Post(s)
| ||||||||
|
Re: What is This Nasty Shit?
An alien laid eggs in him and they are almost ready to hatch.
|
|
#4
●
04-29-2013, 05:47 AM
| ||||||||
| My Rank: FIRST SERGEANT Poster Rank:373 Join Date: Jun 2010 Posts: 3,163 Mentioned: 15 Post(s) Quoted: 882 Post(s)
| ||||||||
|
Re: What is This Nasty Shit?
Looks like a shit load of pussy spots, I have an urge to pop them all |
|
#5
●
04-29-2013, 05:47 AM
| ||||||||
| ★ ********* ★ Poster Rank:246 Male Join Date: Jul 2009 Posts: 5,565
Contributions: 368
Mentioned: 66 Post(s) Quoted: 932 Post(s)
| ||||||||
|
Re: What is This Nasty Shit?
An unusual presentation of primary cutaneous nocardiosis at a rare site: Succesful treatment with a modified Welsh regimen Praveen Kumar S MD DNB, T K Sumathy MD MNAMS, A L Shyam Prasad MD, Gayathri Devi D R MD, K N Shivaswamy MD DNB, C Ranganathan MD DVD Dermatology Online Journal 17 (12): 1 http://dermatology.cdlib.org/1712/1_...6/article.html 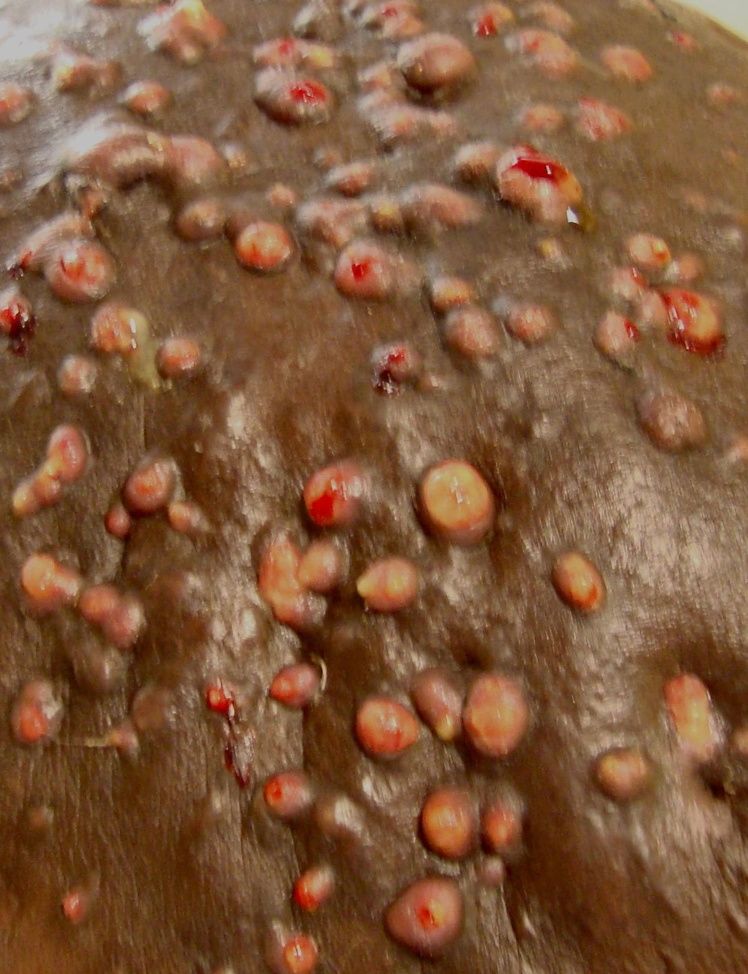 ·  ·  ·  ·  · |
























{kind=link}