|
#1
●
08-23-2024, 08:02 PM
| ||||||||
| These are the rooms Poster Rank:25 of ruin. Join Date: Sep 2014 Posts: 54,011 Mentioned: 145 Post(s) Quoted: 30403 Post(s)
| ||||||||
|
Tonssilar Squamous Cell Carcinoma
In October 2021, a 34-year-old African American male sought medical attention at the Florida Department of Corrections (FDOC) for symptoms involving long-standing bilateral lymphadenopathy, new-onset weight loss, and dysphagia of unknown duration. An initial CT of the neck showed a 5.2 x 5.0 x 4.4 cm mass on the right side. Further imaging via PET scans revealed three enlarged and hypermetabolic lymph nodes in the right neck, showing activity in the tonsils. Subsequent biopsy with p40 immunochemistry staining confirmed squamous cell carcinoma suspected to originate from the tonsils. Further confirmation occurred during the patient's admission to the regional community hospital, where a comprehensive right neck suspension microlaryngoscopy, biopsy, and right tonsillectomy identified a nodular presence in the right tonsil. The investigation revealed invasive squamous cell carcinoma of the right tonsil, with likely cervical nodal metastasis. In February 2022, the patient commenced a regimen of radiation therapy complemented by cisplatin chemosensitization, consisting of 43 sessions targeting the head and neck. Subsequent follow-ups demonstrated a significant reduction in the dimensions of the neck mass, with a near-complete resolution of hypermetabolism in several right neck lymph nodes, indicative of a robust response to therapy. By May 2022, the patient was referred to an otolaryngologist for resection of the last active lymph node in the neck. In the ensuing months, the patient experienced a recurrence of symptoms, including neck pain, swelling, hoarseness, and dysphagia. In October 2022, the patient underwent a radical right neck dissection, although full excision was impeded by the mass's proximity to the carotid paravertebral space. Despite this, the surgical wound demonstrated commendable healing. However, an unforeseen complication emerged several months later, manifesting as an abscess in the remaining tumor tissue. The patient was treated with amoxicillin and clavulanic acid (Augmentin), followed by additional imaging revealing a significant enlargement of the tumor. Immunotherapy with pembrolizumab (Keytruda) was initiated. Despite an initial favorable tolerance, the patient experienced progressive growth of the mass, culminating in complications such as neutropenia and anemia. In November 2023, the patient was admitted to the hospital at the Reception and Medical Center due to the onset of a fever with a white blood cell count of 1,840 cells per cubic millimeter (mm3) and hemoglobin (Hgb) of 6.5 g/dl. On presentation, the patient exhibited a distinct 7 x 7 cm fungating, exophytic mass with fibrinous discharge on the right side of the neck (Figure 1). Cultures from the mass confirmed the presence of Pseudomonas aeruginosa, group A Streptococcus, Escherichia coli, Bacteroides vulgatus, and Enterococcus faecalis. In response to this complex scenario, a range of interventions were employed. This included blood transfusions to address hemoglobin deficits, the administration of Granix to bolster neutrophil counts, and the use of appropriate intravenous antibiotic therapy to combat potential infectious agents. Concurrently, diligent daily wound care protocols were implemented to optimize healing outcomes. As a result, notable improvements were seen in the patient's clinical parameters. The patient’s fever resolved, white blood cells and hemoglobin improved, and repeat blood cultures came back negative with a reduction of suppurative exudate. Maxillofacial specialists at the local academic hospital conducted a thorough evaluation, utilizing a CT scan to unveil the extent of the tumor's invasion into the anterior and posterior neck compartments. The findings revealed invasion into the right carotid space, involving partial encasement and displacement of the right internal and external carotid arteries, along with compression of the right internal jugular vein. Further infiltration extended to the right parotid and masticator spaces, as well as invasion at levels C3-4 and C4-5 into the right paravertebral and perivertebral soft tissues, potentially reaching into the right transverse foramen and causing possible encasement of the distal V2 segment of the right vertebral artery. The assessment also identified soft tissue edema in the hypopharynx, resulting in the narrowing of the supraglottic airway and medialization of the right vocal cord. Considering that the tumor was classified as inoperable, the role of wound care emerged as pivotal in significantly enhancing the patient's comfort and overall well-being. This nuanced care played a crucial role in the patient's comprehensive treatment plan. Strategic wound care was crucial for this patient's outcome. Initial steps involved culturing the wound for pathogen identification and starting broad-spectrum antibiotics until culture results were available. Dakin's 0.50% solution was then used to cleanse the wound and prevent infections. For the unique tumor condition, Santyl (Smith+Nephew, Memphis, TN) therapy removed necrotic tissues, and Xeroform gauze fortified and covered the specific tissue, secured with 4 x 4 sterile gauze, Kerlix wrap, and coverall tape changed daily. This comprehensive approach effectively managed the polymicrobial infection, significantly improving the patient's overall condition. On admission, the patient exhibited a striking 7 x 7 cm fungating, exophytic mass with fibrinous discharge on the right side of the neck (Figure 1). Following four weeks of meticulous wound care, the fibrinous exudate resolved, revealing a pristine expanse of skin primed for regeneration (Figure 2). Prior to wound care, the patient's discomfort and embarrassment were notable, stemming from the unsettling sight, discharge, and odor coming from the wound. The intervention of a wound care specialist significantly enhanced the patient's quality of life by addressing the appearance and odor, resulting in notable improvements.  · 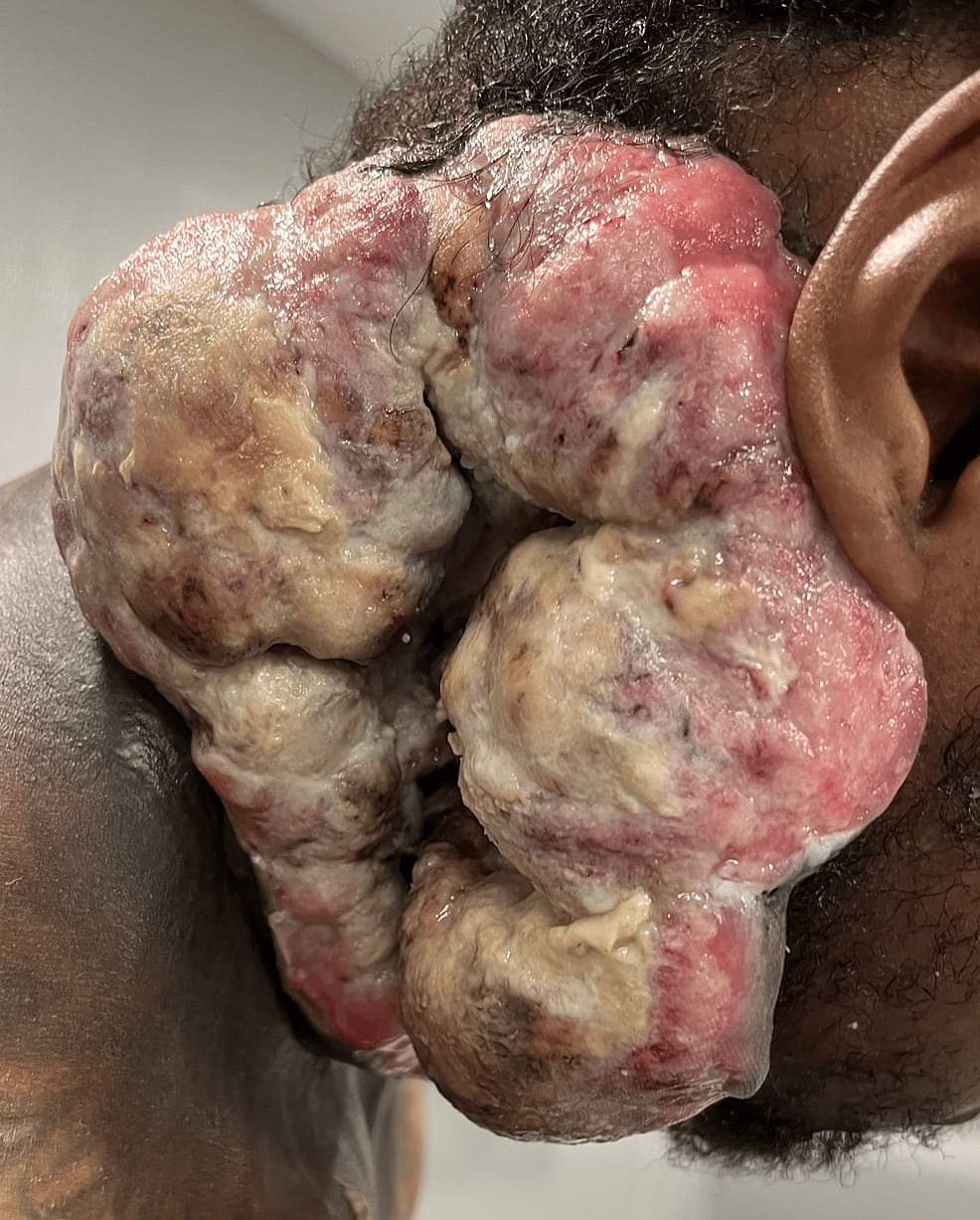 · |
|
#2
●
08-24-2024, 02:41 AM
| ||||||||
 ♚ Legacy Gold Member ♚ Poster Rank:1280 Femme fatale Join Date: May 2024 Posts: 477 Mentioned: 1 Post(s) Quoted: 191 Post(s)
| ||||||||
|
Re: Tonssilar Squamous Cell Carcinoma
That is so gross Looks like he's got dumplings coming out of his neck. |
|
#3
●
08-24-2024, 03:59 AM
| ||||||||
| ★ Legacy Member ★ Poster Rank:119 Secret Agent Join Date: Dec 2009 Posts: 13,207 Mentioned: 6 Post(s) Quoted: 2787 Post(s)
| ||||||||
|
Re: Tonssilar Squamous Cell Carcinoma
Another up and coming “Clicker” These cancers are insane. |
|
#5
●
08-24-2024, 07:48 PM
| ||||||||
| ♚ Legacy Gold Member ♚ Poster Rank:267 ꓕSIꓤIꓕ∀S ϽINOᗡꓤ∀S Join Date: Feb 2010 Posts: 5,101
Contributions: 6
Mentioned: 38 Post(s) Quoted: 1417 Post(s)
| ||||||||
|
Re: Tonssilar Squamous Cell Carcinoma
A prisoner of cancer and the state... ironic.
__________________ ✦ Live life to it's fullest and leave a sexy corpse ✦ |
|
#6
●
08-27-2024, 03:16 AM
| ||||||||
| Wide 'n' sassy Poster Rank:1246 Female Join Date: Mar 2009 Posts: 496 Mentioned: 5 Post(s) Quoted: 69 Post(s)
| ||||||||
|
Re: Tonssilar Squamous Cell Carcinoma
If he was having all that done while still being in jail/prison then he's lucky. As I understand it, correctional facilities in the USA aren't all that generous when it comes to treating illnesses.
|
|
#7
●
10-03-2024, 08:17 PM
| ||||||||
| My Rank: PRIVATE Poster Rank:10566 Female Join Date: Jun 2016 Posts: 13 Mentioned: 0 Post(s) Quoted: 1 Post(s)
| ||||||||
|
Re: Tonssilar Squamous Cell Carcinoma
“Cultures from the mass confirmed the presence of Pseudomonas aeruginosa, group A Streptococcus, Escherichia coli, Bacteroides vulgatus, and Enterococcus faecalis.” |
|
#8
●
10-07-2024, 04:24 AM
| ||||||||
| My Rank: SERGEANT Poster Rank:1101 Female Join Date: Feb 2016 Posts: 594 Mentioned: 0 Post(s) Quoted: 187 Post(s)
| ||||||||
|
Re: Tonssilar Squamous Cell Carcinoma
That's true, however things are getting better. When an addict comes into the prison, and are still using, the prisons now have Methadone/ Suboxone clinics, it's proof that many of these people stay out of prison. Medical care has improved because convicts except for rapists, wife beaters and pedophiles. So they get treated like everyone else
|
|
#10
●
10-07-2024, 11:06 PM
| ||||||||
| ♚ Legacy Gold Member ♚ Poster Rank:267 ꓕSIꓤIꓕ∀S ϽINOᗡꓤ∀S Join Date: Feb 2010 Posts: 5,101
Contributions: 6
Mentioned: 38 Post(s) Quoted: 1417 Post(s)
| ||||||||
|
Re: Tonssilar Squamous Cell Carcinoma
IDK how rapidly this progressed, but there are definitely cases where tumors and infected masses suddenly grow enormous in just a few weeks/months. It would be interesting to find out why he was incarcerated and for how long. If he is serving a life sentence (or capital punishment), then yeah he just waits to die. If not, most states allow prisoners (or conservators) to request compassionate early release if their terminal medical issues can not be adequately addressed by prison physicians, but it's rare. About 75 prisons in USA have hospice centers.
__________________ ✦ Live life to it's fullest and leave a sexy corpse ✦ |































