|
#1
●
10-27-2021, 01:10 PM
| ||||||||
| ♚ Legacy Gold Member ♚ Poster Rank:908 Join Date: Jul 2020 Posts: 820
Contributions: 10
Mentioned: 13 Post(s) Quoted: 173 Post(s)
| ||||||||
|
Reconstruction of Massive Full-thickness Abdominal Wall Defect
In May 2014, a 51-year-old morbidly obese woman (BMI 48), suffering from non-insulin-dependent diabetes, presented at the emergency department with a 20-year-old incisional hernia that had become incarcerated. At admittance, the abdomen was described with horizontal and vertical scars from former surgery and a discolored midline hernia measuring 30 × 50 cm. 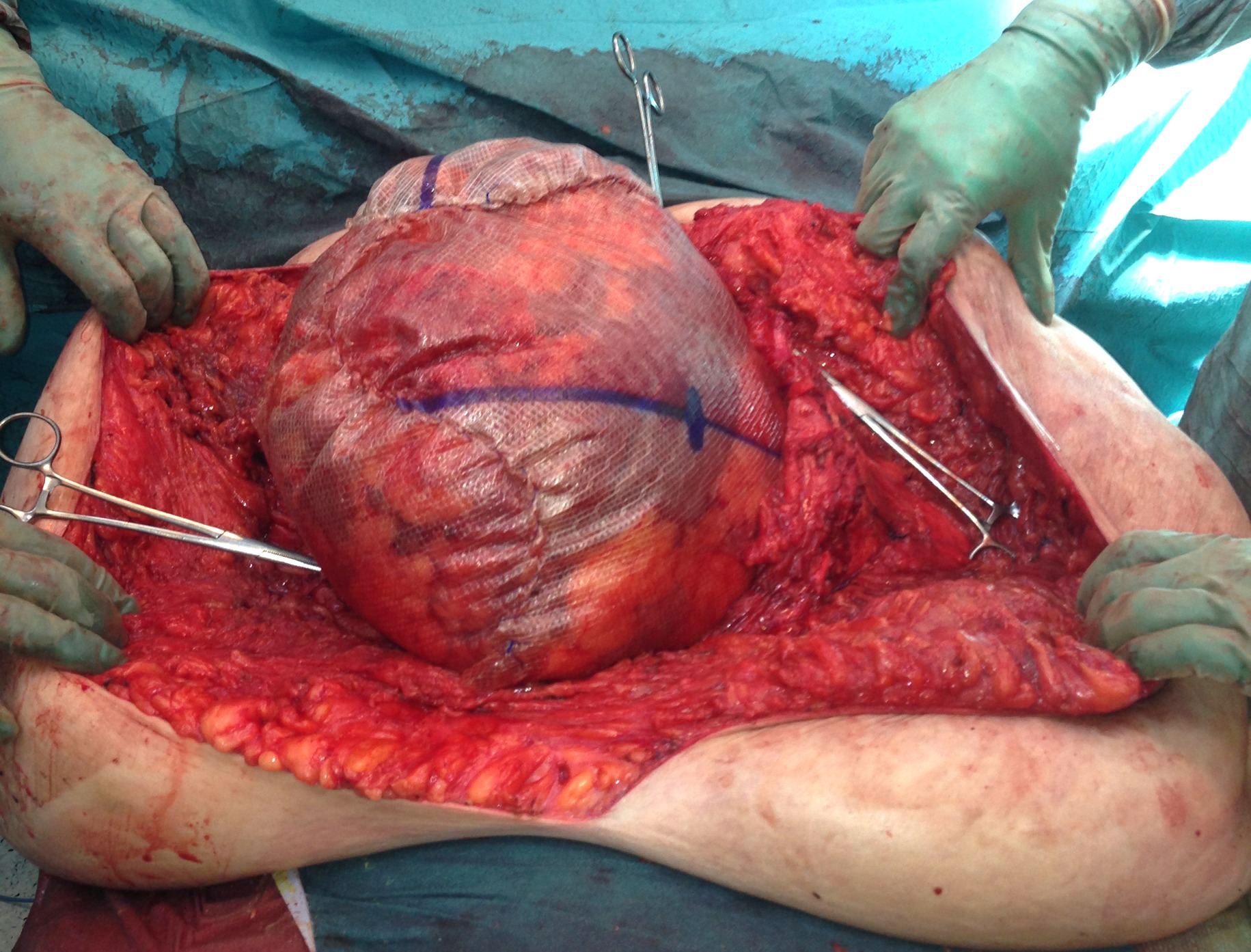 Fig.1 Perioperative photograph with three pieces of synthetic mesh sewn together and to the facial edges (shown with peans) to substitute the abdominal wall.  Fig.2 After eight months of VAC treatment and just prior to split-skin transplantation. Note the mesh is almost invisible and the abdominal skin has reattached to the lateral aspects of the truncus. Acute CT of the abdomen demonstrated small bowel obstruction, and an immediate explorative laparotomy was performed via the vertical scar. Perioperatively, the abdominal wall defect measured 15 × 10 cm, and the ventricle, colon, and small intestine were encapsulated in a subcutaneous cavity. The lower 150 cm of the small intestine was cyanotic and torqued around the mesentery; detorquing resulted in revitalization.  Fig.3 One week after split-skin transplantation. Note good graft take, folding of the mesh in the upper aspect of the defect and yellow secretion from what turned out to be a high small bowel fistula with low output.  Fig.4 Two months after split-skin transplantation. The inset photograph six weeks after transplantation. Huge amount of mesh eroded through the transplanted skin and cut off successively. The intra-abdominal cavity was found shrunken and too small to contain the intestinal organs. Consequently, the fascia was split proximally and distally of the hernia port; however, the abdominal wall could not be closed without the use of three pieces of nonabsorbable mesh each measuring 35 × 35 cm (Fig. 1). The intra-abdominal organs were enclosed in the new cavity, and the skin was closed above the cavity.  Fig.5 Nine months after skin transplantation. The patient is almost healed. Inset: 28 months after the hernia operation and 20 months after the skin transplantation. A chronic skin defect in the right lateral groove, presumably due to the heavy weight of the lateral role and mechanical collision. - This post is for educational purposes only and is nonprofit. Under Section 107 of the US Copyright Act of 1976; Allowance is made for "Fair Use" for purposes such as criticism, comment, news reporting, teaching, scholarship, and research. OP is not a medical expert. No copyright infringement intended. This post does not encourage or glorify violence/harassment. Images might have been upscaled and enhanced. Text might have been shortened and simplified/reorganized for online view. |
|
#2
●
10-27-2021, 01:48 PM
| ||||||||
| ★ Legacy Member ★ Poster Rank:248 So many choices now Join Date: Jul 2015 Posts: 5,548 Mentioned: 15 Post(s) Quoted: 2120 Post(s)
| ||||||||
|
Re: Reconstruction of Massive Full-thickness Abdominal Wall Defect
Michelin Man's mother.
|
|
#4
●
10-27-2021, 06:32 PM
| ||||||||
| ♚ Legacy Gold Member ♚ Poster Rank:842 Join Date: Apr 2016 Posts: 911 Mentioned: 1 Post(s) Quoted: 156 Post(s)
| ||||||||
|
Re: Reconstruction of Massive Full-thickness Abdominal Wall Defect
Our bodies are not meant to be that obese. This whole situation is just wrong. |
|
#5
●
10-28-2021, 03:33 AM
| ||||||||
 ★ Legacy Member ★ Poster Rank:772 I'm not A bitch.... I'm THE bitch. Join Date: Jul 2012 Posts: 1,033 Mentioned: 4 Post(s) Quoted: 174 Post(s)
| ||||||||
|
Re: Reconstruction of Massive Full-thickness Abdominal Wall Defect
She needs to go fucking exercise…..or get her feet out from under the dining table.
|
|
#6
●
10-28-2021, 08:16 AM
| ||||||||
| My Rank: LANCE CORPORAL Poster Rank:2259 Join Date: May 2012 Posts: 206 Mentioned: 0 Post(s) Quoted: 57 Post(s)
| ||||||||
|
Re: Reconstruction of Massive Full-thickness Abdominal Wall Defect
She suffered from an over active knife and fork
|
|
#8
●
11-01-2021, 03:52 AM
| ||||||||
| ♚ Legacy Gold Member ♚ Poster Rank:195 Female Join Date: Nov 2009 Posts: 7,761 Mentioned: 5 Post(s) Quoted: 708 Post(s)
| ||||||||
|
Re: Reconstruction of Massive Full-thickness Abdominal Wall Defect
THIS. I work in a hospital and we have to hoist these people and roll them, etc. Takes 6 nursing staff sometimes. And UK isn’t quite as obese as USA. Yet. |
|
#9
●
11-01-2021, 04:22 PM
| ||||||||
| My Rank: LANCE CORPORAL Poster Rank:2057 Female Join Date: May 2013 Posts: 238 Mentioned: 0 Post(s) Quoted: 56 Post(s)
| ||||||||
|
Re: Reconstruction of Massive Full-thickness Abdominal Wall Defect
You get 6 staff and a hoist??? Lucky bugger.
|
|
#10
●
11-26-2021, 07:25 PM
| ||||||||
| ♚ Legacy Gold Member ♚ Poster Rank:67 Join Date: Jul 2008 Posts: 23,776 Mentioned: 94 Post(s) Quoted: 12346 Post(s)
| ||||||||
|
Re: Reconstruction of Massive Full-thickness Abdominal Wall Defect
stop fat shaming. BMI is just a construct made up by gym companies
|































{kind=link}