|
#1
●
10-27-2010, 12:33 AM
| ||||||||
| ★ realist-absurdist ★ Poster Rank:139 female Join Date: Feb 2010 Posts: 11,717 Mentioned: 0 Post(s) Quoted: 16 Post(s)
| ||||||||
|
Rebuilding His Cancerous Nose from His Forehead
{I found this to be quite interesting- he goes thru a rather bizarre process and ends up looking normal & healthy ... I hope the photos embed in proper order to coincide with the 1-15 explanations} Media file 1: Recurrent basal cell carcinoma is present within parts of the left dorsum, tip, and ala. Both rims are significantly retracted due to previous cancer excisions. Media file 2: After Mohs excision, an extensive defect of the dorsum, tip, ala, sidewall, and medial cheek is present. Note that the right rim remains significantly retracted due to scar from previous skin cancer treatment. Media file 3: The nasal subunits are marked. Media file 4: An incision is made in the right alar crease and after releasing the retracted right ala and bracing the sidewall with a primary cartilage graft, the right cheek is advanced to supply missing skin to the sidewall. The right ala is repositioned. The left cheek defect is repaired using a superior, laterally based cheek flap with an incision in the left nasolabial fold. A primary conchal cartilage graft is positioned to support, shape, and brace the left soft triangle and alar subunits. Media file 5: Residual normal skin within the tip and left alar subunits is excised, altering the wound so that nasal subunits will be reconstructed rather than the defect just "filled". The left alar lining is supported by a primary conchal cartilage graft. Media file 6: A full thickness left paramedian forehead flap based on an exact template is transposed to the nasal defect. The gap that remains in the forehead after partial closure is allowed to heal secondarily. Media file 7: Adjacent normal skin within the tip and left ala was excised and the nose resurfaced as subunits. The forehead flap resurfaces most of the dorsum, all of the tip, left sidewall, and ala. A left cheek flap was rotated and advanced to resurface the cheek defect. Media file 8: At three weeks, the reconstruction is bulky. Although periosteum has desiccated, the forehead donor site continues to heal secondarily. Media file 9: At an intermediate operation, three weeks after initial forehead flap transfer, the forehead flap is re-elevated with 2-3 mm subcutaneous tissue and temporarily placed to the side. The underlying excess subcutaneous tissue, frontalis muscle and scar are exposed and marked for excision. Media file 10: Excess subcutaneous fat and frontalis are exposed. Nasal subunits are outlined with ink. Media file 11: A sculptured nasal shape is created by excision of excess soft tissues. Forehead skin of uniform nasal "thinness" is returned to the nasal recipient site and fixed with quilting and peripheral sutures along its margins. Media file 12: At six weeks, the forehead defect continues to heal. The nose is assuming a better nasal shape. Media file 13: At the third stage, six weeks after initial flap transfer, the pedicle is divided, the proximal aspect is thinned and re-inset in the inferior forehead as a small inverted "V". The distal flap is elevated with a few millimeters of subcutaneous tissue, exposing residual excess soft tissue in the most proximal aspects of the repair which is excised to recreate the subtle dorsal lines, a flat nasal sidewall, and a more defined alar crease. Media file 14: Excess skin is excised and the wound is sutured with quilting and peripheral sutures. Media file 15: Eight months after repair without revision, the forehead defect has healed secondarily with minimal scarring. A good nasal shape has been restored. Distortions of the ala from previous surgeries have been fully corrected. Forehead, right and left nasolabial scars are virtually invisible. 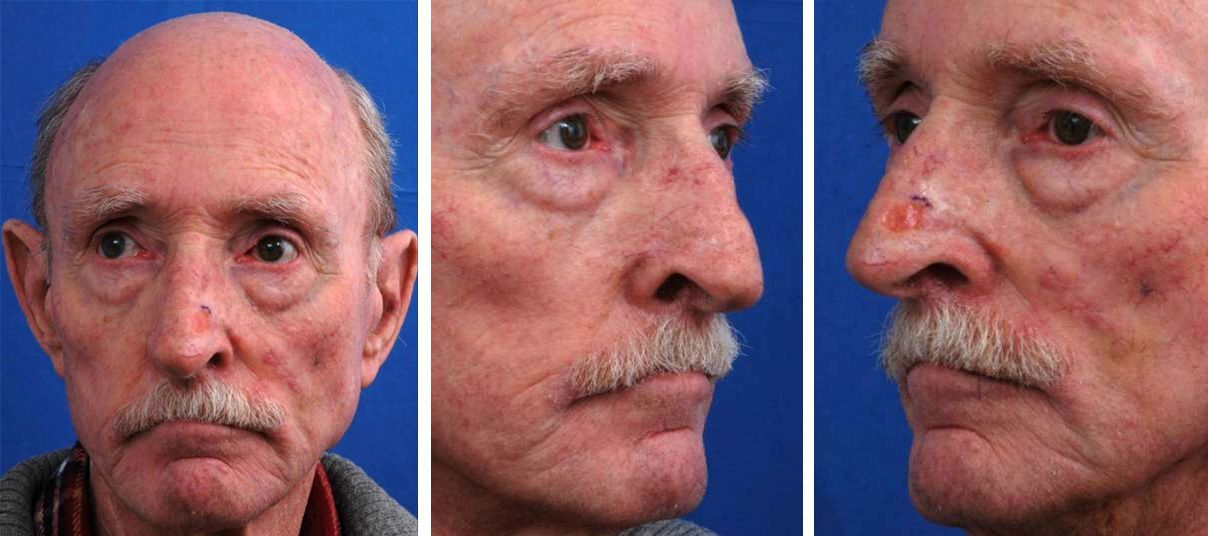 ·  · 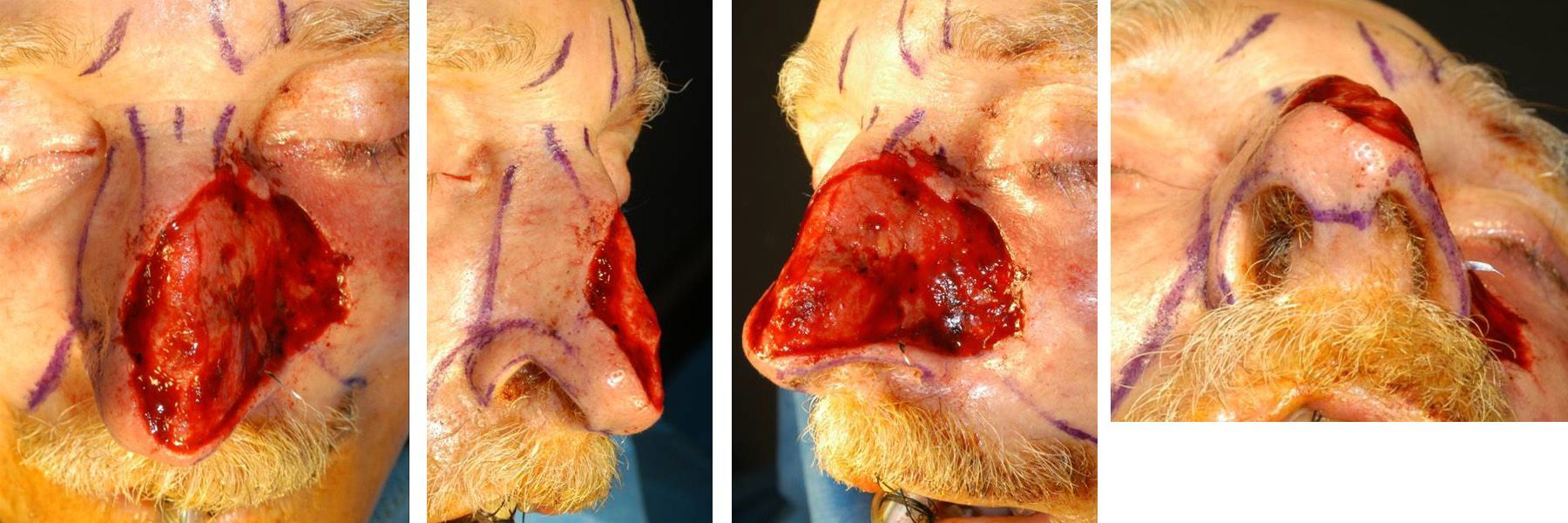 · 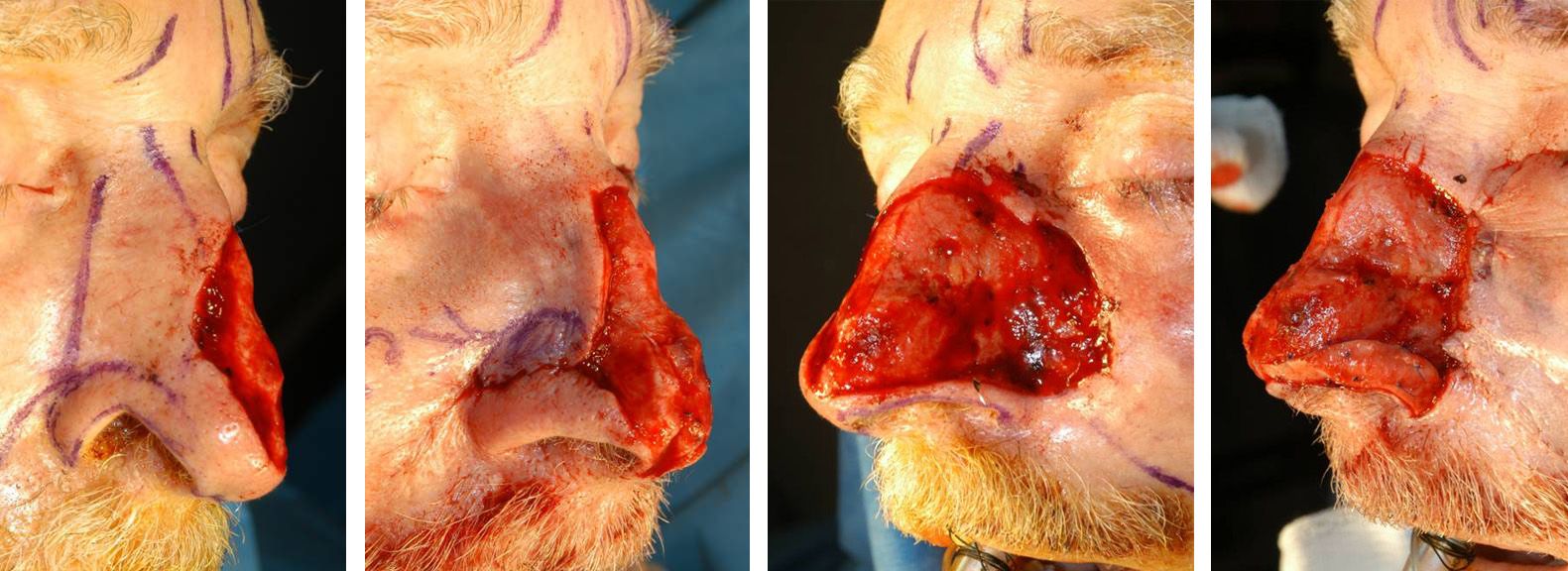 · 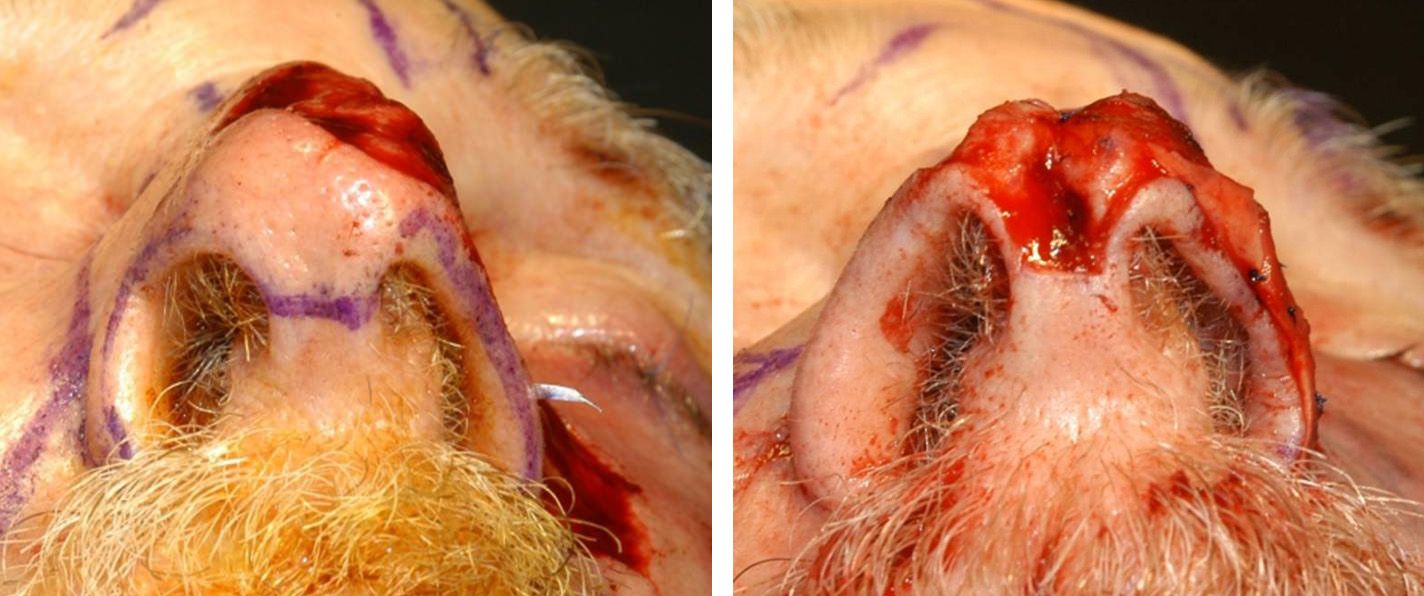 ·  ·  ·  ·  · 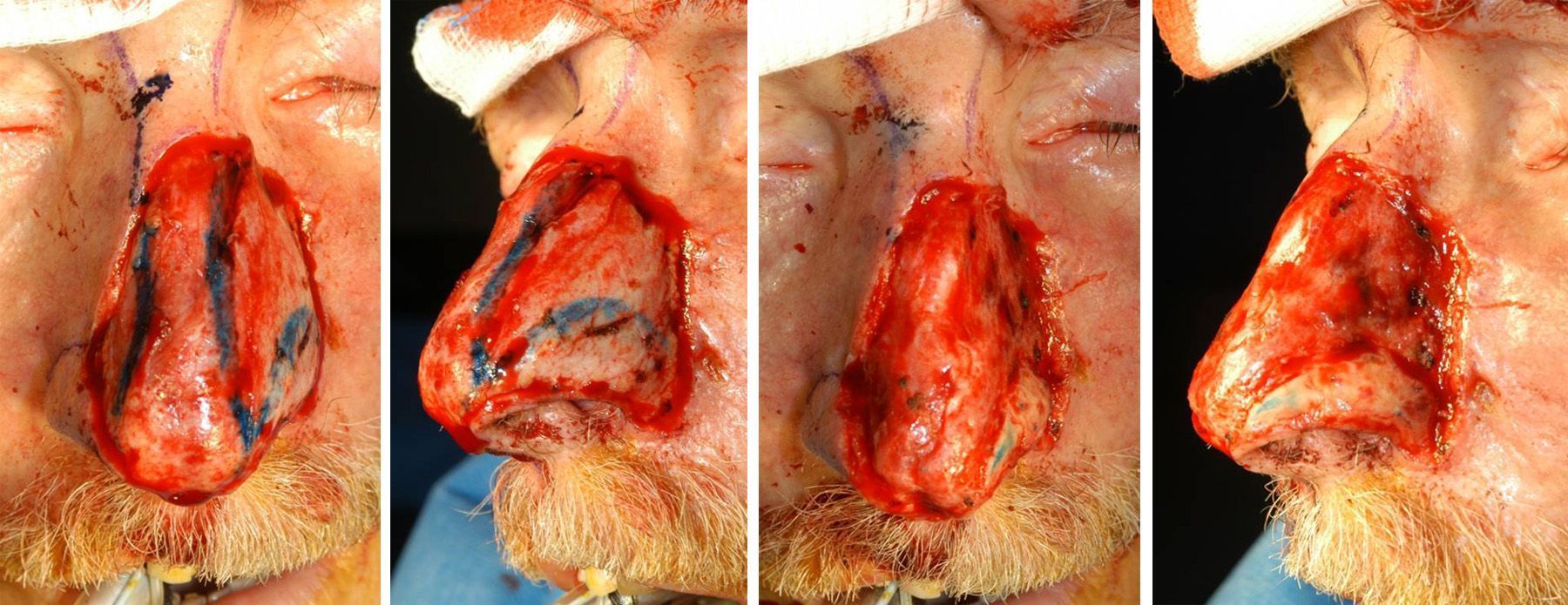 ·  · 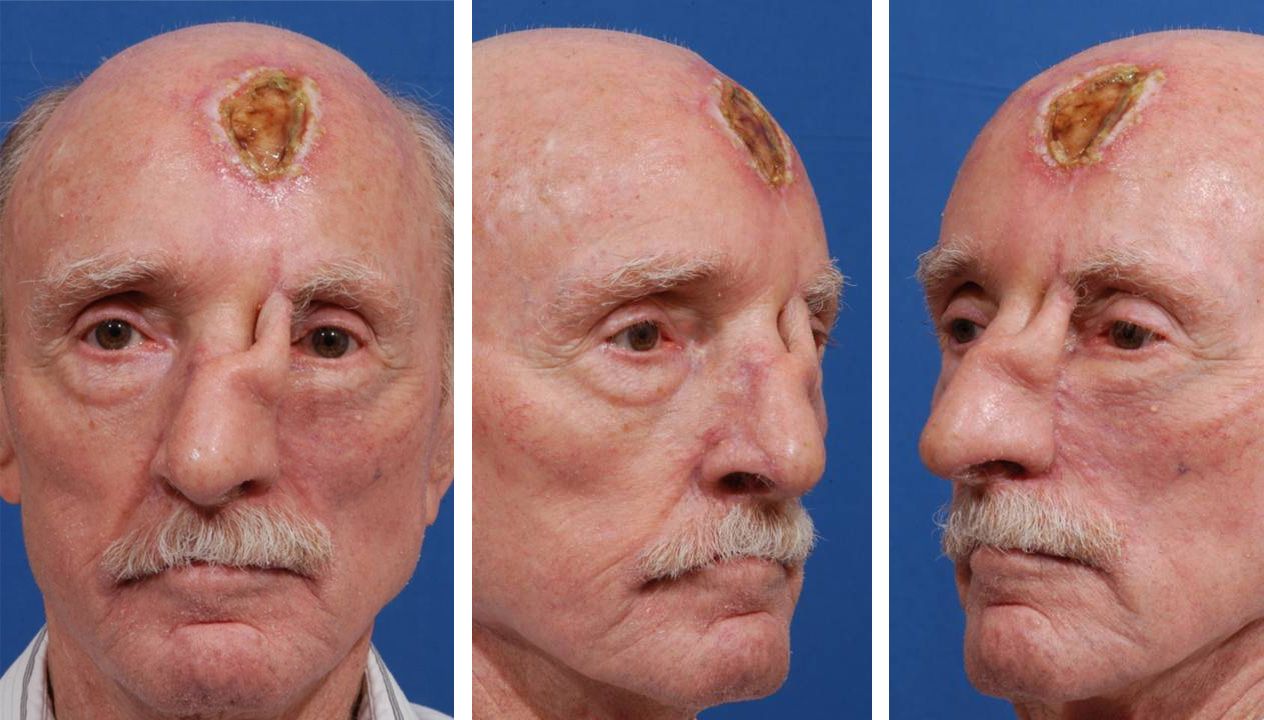 · 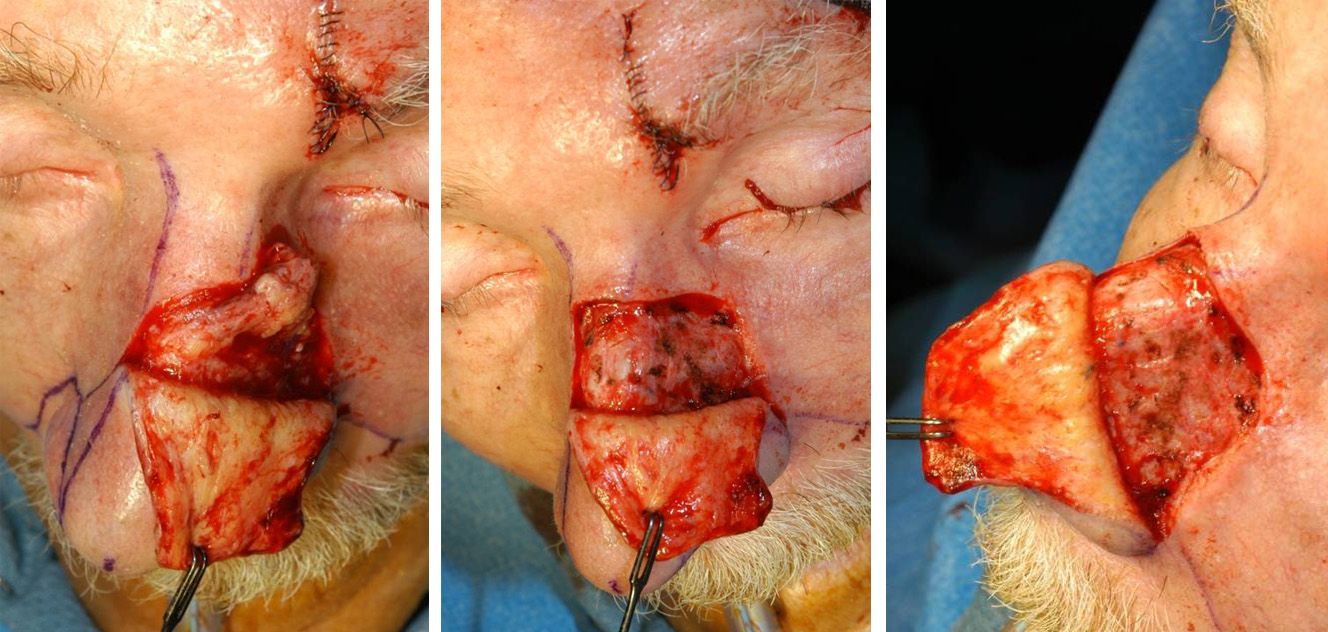 ·  ·  · |
|
#7
●
10-27-2010, 11:43 PM
| ||||||||
| My Rank: MASTER SERGEANT Poster Rank:582 Male Join Date: Aug 2009 Posts: 1,634
Contributions: 1
Mentioned: 0 Post(s) Quoted: 177 Post(s)
| ||||||||
|
Re: Rebuilding His Cancerous Nose from His Forehead
Wow, I wouldn't realize he went through all that if someone showed me the final picture. Amazing. |






















{kind=link}