|
#1
●
03-27-2023, 10:44 PM
| ||||||||
| These are the rooms Poster Rank:25 of ruin. Join Date: Sep 2014 Posts: 54,011 Mentioned: 145 Post(s) Quoted: 30403 Post(s)
| ||||||||
|
Multiple Myeloma of the Scalp
Source: A 63-year-old woman was transferred to our department with a large fungating tumor of the left temporo-parietal scalp diagnosed as MM presenting as an EMP. Three months earlier, she underwent an excisional biopsy of a slow-growing, subcutaneous nodule on the left frontoparietal aspect of her scalp. The lesion was 1 cm in diameter, purplish in color, firm to the touch, and mobile. The pathologic findings led to the initial diagnosis of plasmacytoma, after which the patient underwent a full hematological workup. The disease was oligosecretory, with no para-proteinemia and a monoclonal population of plasma cells occupying about 30% of the bone marrow cells. PET-CT demonstrated two additional bony lesions in the left 4th rib with an expanding soft-tissue mass and in the 11th thoracic vertebra. Her final diagnosis was summarized as MM with an extramedullary plasmacytoma. Within several weeks following the initial biopsy, the scalp lesion grew rapidly in the scar, reaching a size of 10 cm in diameter. It spread to the adjacent calvaria creating a full-thickness defect 3 cm in diameter. The lesion was painful, highly vascular with multiple necrotic foci and oozed blood uncontrollably (Figure 1). Palliative radiotherapy (16 Gy in four fractions) was initiated in attempt to control the bleeding but failed to do so. The patient's hemoglobin levels dropped steadily to 6.5 mg/dL, necessitating multiple blood transfusions. Another therapeutic attempt was made, and the patient received two cycles of chemotherapy with bortezomib, cyclophosphamide, and dexamethasone (VCD) with no observable response. At this point, the patient was transferred to a tertiary facility, where a multidisciplinary team was formed and included hemato-oncologists, radiation oncologists, neurosurgeons, and plastic surgeons. It was felt that the medical treatment for the imminent terminal scalp lesion was exhausted, and therefore, a surgical approach was decided upon. A collaborative approach consisting of neurosurgery performing a wide resection of the tumor and plastic surgery immediately reconstructing the skull and scalp defect. The preoperative evaluation included a head CT that demonstrated a 4.1 × 11 × 10 cm space-occupying lesion in the soft tissue of the scalp with a bone defect of 2.7 × 1.2 × 2.4 cm. The lesion contained multiple hemorrhagic foci, and an MRI study showed homogeneous enhancement of the dura underneath it, suggesting its involvement (Figure 2). A biopsy was obtained from the lesion and showed large cells with plasmoblastic differentiation. The patient underwent surgery within a week of her transfer (Figure 3). The tumor was resected with 2-cm skin margins, and a wide craniectomy was performed leaving a bony defect of about 5 cm in diameter. The dura did not appear to be involved macroscopically and was therefore left intact. Intraoperative frozen sections were sent for pathologic analysis. The skin showed anaplastic plasmacytoma with resection margins free of tumor. The tumor itself consisted of sheets of pleomorphic cells with an increased mitotic rate. The tumor cells were positive for CD56, CD79a, CD138, and lambda light chains, and negative for CD20, IgM, and kappa light chains. Eighty percent of the cells were positive for Ki-67.11, 12 The bony defect was covered with a titanium mesh, and soft tissue was reconstructed using a latissimus dorsi muscle free flap covered by a split-thickness skin graft. Anastomoses were performed in an end-to-end fashion between the thoracodorsal vessels and the left superficial temporal vessels. Ischemia time was 90 minutes. The postoperative period was totally uneventful, the skin graft had taken completely, and the patient recovered rapidly with no medical, neurological, or surgical sequelae (Figure 4). She was discharged on postoperative day 15 with a stable hemoglobin level of 9.9 mg/dL. Three weeks postoperatively, she began biologic therapy with dexamethasone and Velcade (bortezomib), which she tolerated well. She also received electron beam radiotherapy of 15 Gy in five fractions which was started 5 weeks after surgery, and it had no adverse influence on the surgical outcome. At this point, the patient underwent a second PET-CT which demonstrated a new 1.4 cm FDG avid cervical lymph node. A biopsy revealed immature monoclonal plasma cells, and the patient was subsequently treated with high-dose melphalan and autologous HSCT with resolution of the cervical lymphadenopathy. Treatment with lenalidomide, carfilzomib, and dexamethasone was later initiated. The patient continued hematology follow-up and treatment however approximately 18 months following surgery succumbed to the disease.  ·  ·  · 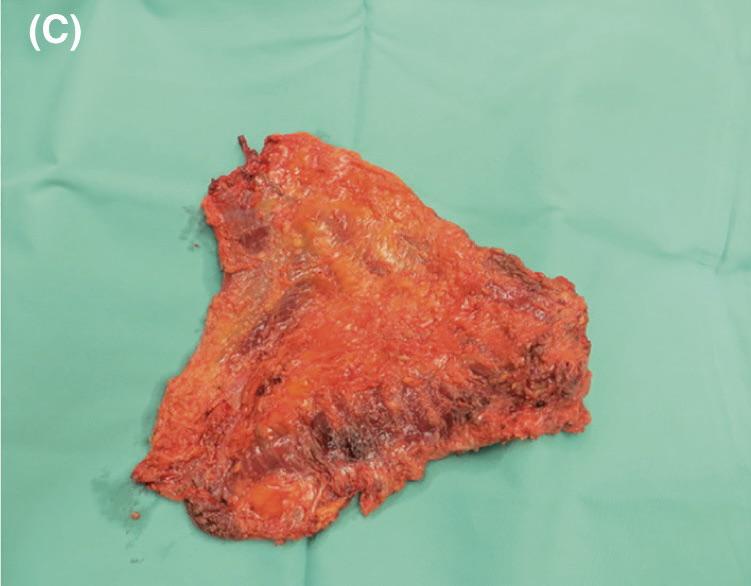 · 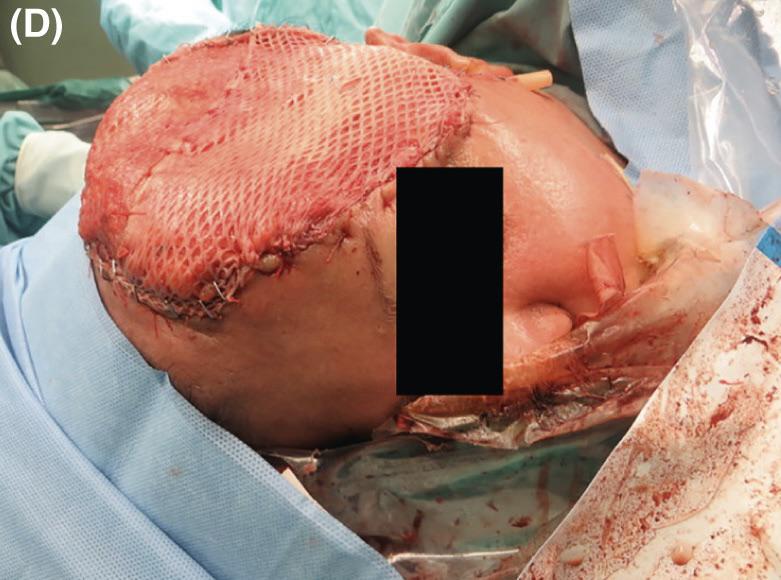 ·  · |
|
#2
●
03-27-2023, 11:32 PM
| ||||||||
| ★ Legacy Member ★ Poster Rank:248 So many choices now Join Date: Jul 2015 Posts: 5,548 Mentioned: 15 Post(s) Quoted: 2120 Post(s)
| ||||||||
|
Re: Multiple Myeloma of the Scalp
That second one looked like a pizza dough bubble.
|
|
#3
●
03-28-2023, 02:40 AM
| ||||||||
| My Rank: FIRST SERGEANT Poster Rank:394 Join Date: Apr 2011 Posts: 3,054 Mentioned: 2 Post(s) Quoted: 276 Post(s)
| ||||||||
|
Re: Multiple Myeloma of the Scalp
And the first one looks like a strawberry jam roll. Maybe a bit scorched and misshapen one, but a jam roll anyways |
























{kind=link}