|
#1
●
04-04-2023, 11:36 PM
| ||||||||
| These are the rooms Poster Rank:25 of ruin. Join Date: Sep 2014 Posts: 54,011 Mentioned: 145 Post(s) Quoted: 30403 Post(s)
| ||||||||
|
He's a Grower Not a Shower.
Source: A 57-year-old man presented to our institution with an irreducible, giant right inguinoscrotal hernia which had been previously reducible and slowly enlarging over many years. This was associated with pain, nausea, and vomiting. He was an ex-smoker of 10 pack-years, but had no other relevant medical or surgical history. On examination, he was hemodynamically stable and afebrile. The abdomen was soft, mildly distended, with no tenderness on palpation. A giant right inguinoscrotal hernia was evident, which extended below the midpoint of his inner thigh (Figure 1). The overlying skin was tender, firm, and erythematous. Blood tests showed a raised c-reactive protein of 300 mg/L with a normal white cell count of 9.8x109/L, and an acute renal injury with creatinine of 177 µmol/L and estimated glomerular filtration rate of 36 mL/min/1.73 m2. Given the clinical concern for bowel obstruction and ischemia, this patient proceeded to urgent operative management without imaging. He underwent an open right hernia repair via Lichtenstein approach. The hernia sac revealed acute appendicitis and a contained abscess, along with fibrinous adhesions to the cecum, terminal ileum, proximal descending colon, and bladder edge (Figures 2, 3). The wound was protected and an appendicectomy was performed with a gastrointestinal anastomosis 80 mm stapler. The staple line was oversewn with 3-0 vicryl and the remainder of the hernial contents were inspected to ensure there was no additional pathology. The giant hernial sac and an Alexis wound retractor were used to contain any contamination as 3 L of saline wash was applied. This was performed until clear returns were seen. Next, the excess hernia sac was excised, and the remainder closed with 2-0 vicryl. The posterior wall of the inguinal canal was plicated with 2-0 vicryl, and the repair was reinforced with ULTRAPRO® partially absorbable mesh (Ethicon Inc., Somerville, NJ). The external oblique aponeurosis and subcutaneous space were closed with 2-0 vicryl. The right testicle was confirmed viable, and a 15 Fr Blake® drain (Ethicon Inc., Somerville, NJ) was inserted into the right scrotum. Local anesthetic was infiltrated and the skin was closed with staples. The patient was admitted to the Intensive Care Unit (ICU) post-operatively due to oligoanuric renal failure. This was likely due to acute tubular necrosis, secondary to obstruction and hypovolaemia. His renal function improved post-operatively with additional fluid rehydration. He was stepped down from ICU on day two post-operatively, and completed five days of intravenous ceftriaxone and metronidazole before being discharged home on oral antibiotics, as per infectious diseases advice. The right scrotal drain remained in situ on discharge to prevent post-operative seroma formation. The patient was also educated on compliance with scrotal support underwear and to avoid heavy lifting or straining. Histopathology of the appendix confirmed acute appendicitis, with transmural inflammatory infiltrate and a meso-appendiceal abscess. The patient recovered well, with improvement in renal function on one-week follow-up. His drain and skin staples were removed uneventfully following this. On four-week follow-up, he remained well with no hernia recurrence.  · 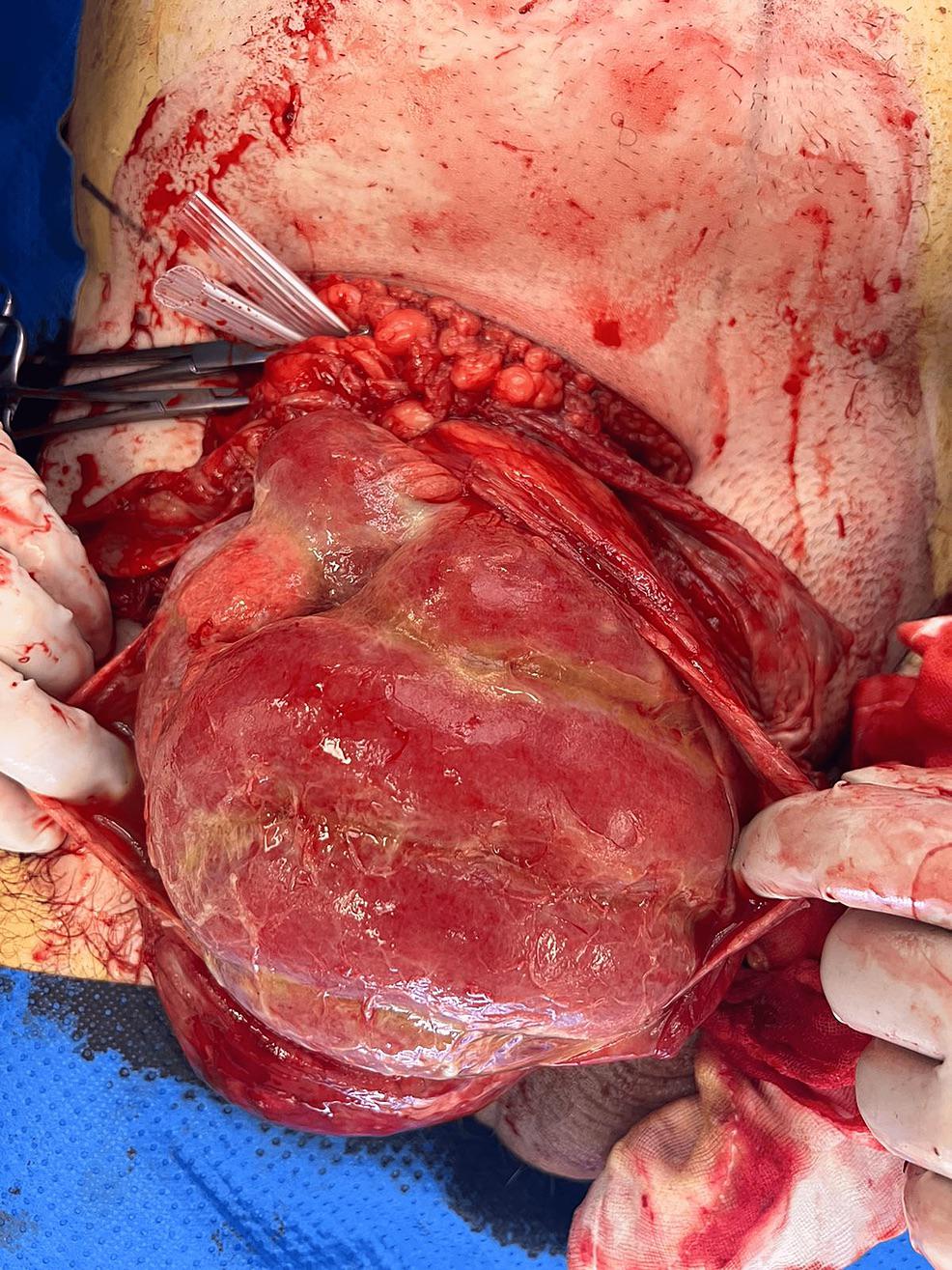 · 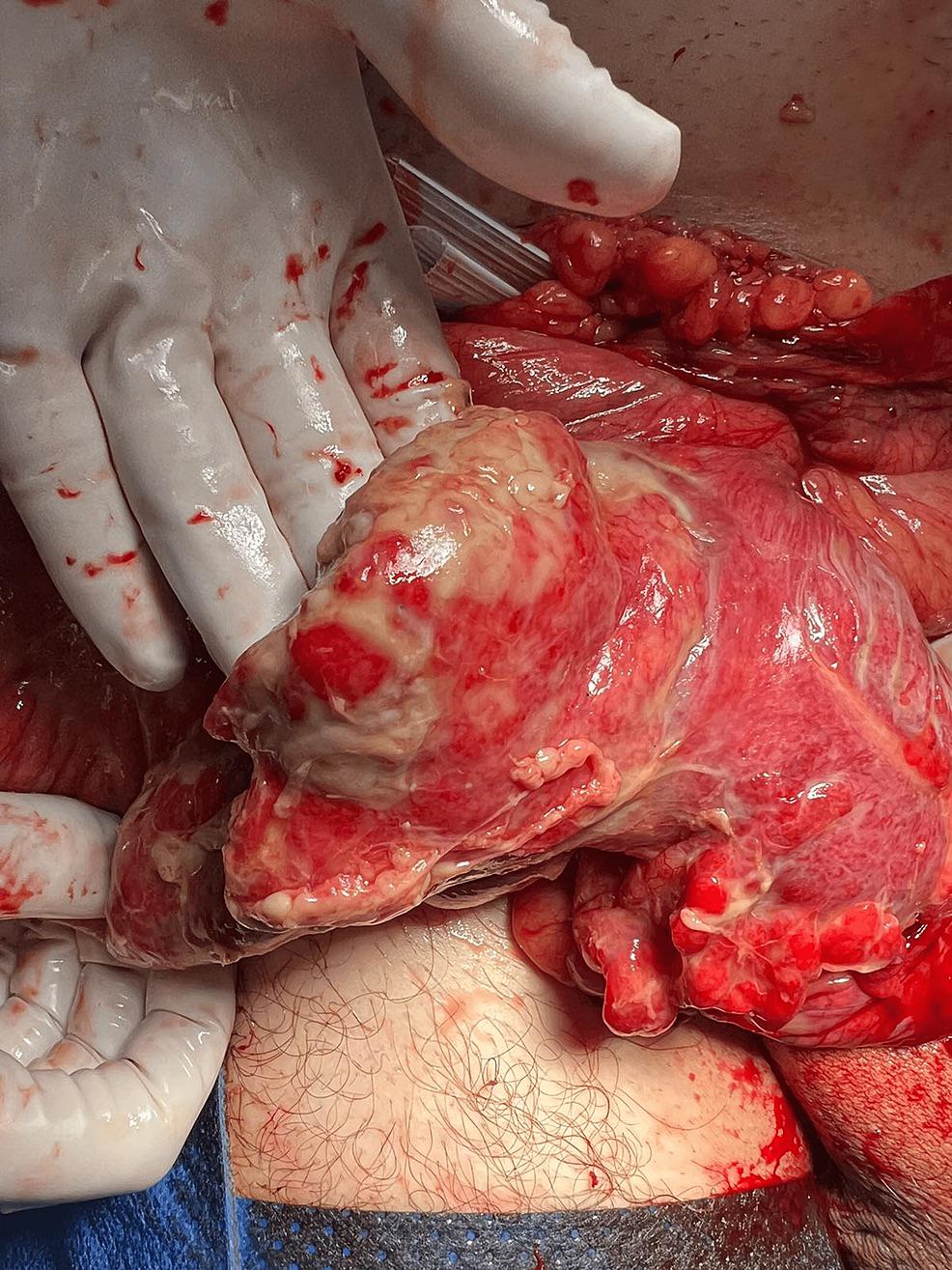 · |
|
#2
●
04-04-2023, 11:42 PM
| ||||||||
| ★ Legacy Member ★ Poster Rank:247 So many choices now Join Date: Jul 2015 Posts: 5,548 Mentioned: 15 Post(s) Quoted: 2120 Post(s)
| ||||||||
|
Re: He's a Grower Not a Shower.
If I like this post, does that mean I'm gay? |
|
#3
●
04-05-2023, 05:40 PM
| ||||||||
| ✝Mudderator from Hell✝ Poster Rank:10 e-mail Join Date: Oct 2006 Posts: 94,975
Contributions: 817
Mentioned: 472 Post(s) Quoted: 10078 Post(s)
| ||||||||
|
Re: He's a Grower Not a Shower.
no, just bi-curious |
|
#6
●
04-06-2023, 05:28 AM
| ||||||||
| My Rank: FIRST SERGEANT Poster Rank:406 Male Join Date: Nov 2009 Posts: 2,957 Mentioned: 18 Post(s) Quoted: 447 Post(s)
| ||||||||
|
Re: He's a Grower Not a Shower.
I had a hernia years back... Called myself E.T. The extra testicle. |



























