|
#1
●
06-06-2024, 02:23 AM
| ||||||||
| These are the rooms Poster Rank:25 of ruin. Join Date: Sep 2014 Posts: 54,011 Mentioned: 145 Post(s) Quoted: 30403 Post(s)
| ||||||||
|
Head Ulcer
A 71-year-old man presented to the emergency room with loss of consciousness after he was found to have drowned in a river. Upon presentation, initial examinations and investigations revealed an E1V1M5 score on the Glasgow Coma Scale, anemia, hyperammonemia, severe inflammation, electrolyte disturbance, hepatic dysfunction, and hypoalbuminemia. He had lacerations on his face, bilateral pneumothorax, multiple rib fractures, and mediastinal emphysema. Therefore, the patient underwent resuscitation after being diagnosed with shock. One of the most conspicuous signs on his body was the presence of a large periosteal defect of the head filled with malodorous necrotic tissue and slough (Fig. (Fig.1).1). A bacterial culture of samples from the head ulcer was positive for Fusobacterium gonidiaformans, Staphylococcus aureus, and Aeromonas species, all of which had been reported to cause necrotizing fasciitis.1–3 Three days after hospitalization, history obtained from the patient revealed a suicidal intent due to pessimism about his general fatigue and economic conditions. According to the CT scan findings, no major injuries were present in the brain. However, a psychiatry consultation to obtain a detailed history was indicated. Subsequently, the consultation revealed a history of ulcer on the head, resulting from a head injury due to a fall from a bridge, which occurred approximately 10 years ago. Two weeks before the drowning event, he had a sense of malaise and episodes of vomiting. Since more than two-thirds of the cranium was covered with grimy and necrotic tissues, extensive debridement was necessary before mapping biopsies. The first mapping biopsy yielded basal cell carcinoma (BCC) in one sample from the temporal skin and actinic elastosis in samples obtained from all other regions. A whole-body CT scan did not show any suspicious mass to be metastatic. Therefore, a second mapping biopsy, with a focus on the temporal regions, was performed under local anesthesia to determine the extent of resection. A radical resection under general anesthesia was performed with a 5-mm margin from the ulcer or BCC-positive area. The left external auricle was resected, whereas the BCC-negative regions, periosteum, and temporal muscle fibers were preserved. Thereafter, the large defect was reconstructed using a meshed split-thickness skin graft (STSG), which was 12 thousandths of an inch in thickness, obtained from the right thigh. Five months after the radical resection, the patient presented with ulcers surrounded by melanotic macules at the outpatient department (Fig. (Fig.2).2). The pathological examination revealed a recurrence of BCC. A head and neck CT scan showed the presence of a subcutaneous nodule in the temporal region without lymphadenopathies. Therefore, a second radical resection of the subcutaneous nodule, temporal muscle, residual periosteum, external table of the skull, and grafted skin was performed. Eight samples of these tissues were sent for pathological examinations, which revealed the presence of BCC in the subcutaneous nodule but not the other tissues. This result indicated that radical dissection was performed with a sufficient margin in the cranium. The defect was reconstructed using a latissimus dorsi (LD) muscle flap, the vessels of which were anastomosed with the superficial temporal artery, the superficial temporal vein, and a subcutaneous vein. The 26 cm × 8 cm skin island over the flap was separated to create a meshed graft at a ratio of 1:3 for covering the LD muscle body (Fig. (Fig.3).3). The graft and flap were taken, and no suspicion or sign of recurrence has been found 6 months after the last operation (Fig. (Fig.44).  ·  · 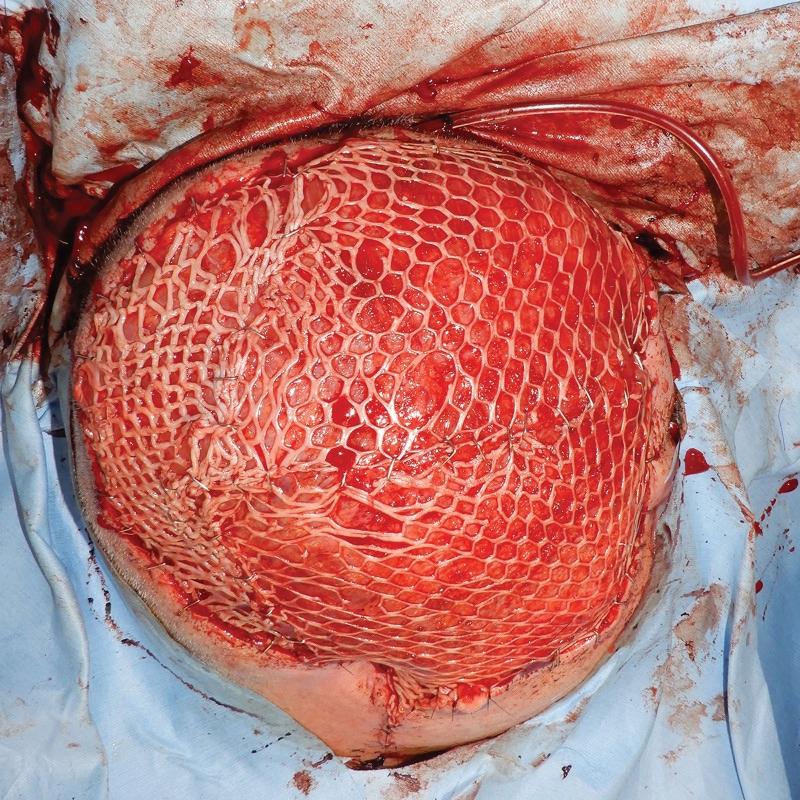 ·  · |
|
#3
●
06-06-2024, 08:07 AM
| ||||||||
| ★ Legacy Member ★ Poster Rank:248 So many choices now Join Date: Jul 2015 Posts: 5,548 Mentioned: 15 Post(s) Quoted: 2120 Post(s)
| ||||||||
|
Re: Head Ulcer
Nice of them to keep the ear hole, such as it is. Looks a bit small for a q-tip.
|
























{kind=link}