|
#1
●
07-05-2012, 08:20 AM
| ||||||||
| My Rank: MAJOR Poster Rank:11 Join Date: Jun 2009 Posts: 93,130
Contributions: 226
Mentioned: 91 Post(s) Quoted: 2009 Post(s)
| ||||||||
|
Emergency Bedside Thoracotomy
Emergency department thoracotomy (EDT, shown) is a very controversial but potentially lifesaving procedure for a select group of patients with blunt and penetrating thoracic trauma. EDT technique has remained fairly unchanged; however, the indications for performing an EDT remain a source of controversy in the literature. The decision to perform an EDT is determined by the presence of signs of life and the mechanism and location of injury. EDTs are successful in ~35% of patients arriving in shock with a penetrating cardiac wound (~15% for all penetrating wounds). Patient outcome is poor (≤2%) when EDT is performed for blunt trauma. 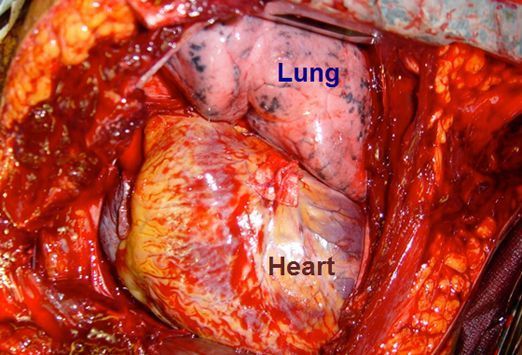 The primary goals of EDT include hemorrhage control, release of cardiac tamponade, facilitation of internal/open cardiac massage, prevention of air embolism, and exposure of the descending thoracic aorta for cross-clamping. EDT is contraindicated for patients with penetrating trauma who undergo cardiopulmonary resuscitation for more than 15 minutes with no signs of life. EDT is contraindicated for patients with blunt trauma who undergo cardiopulmonary resuscitation for more than 5 minutes with no signs of life or asystole. It is also contraindicated for patients with multiple blunt trauma or severe head injuries. 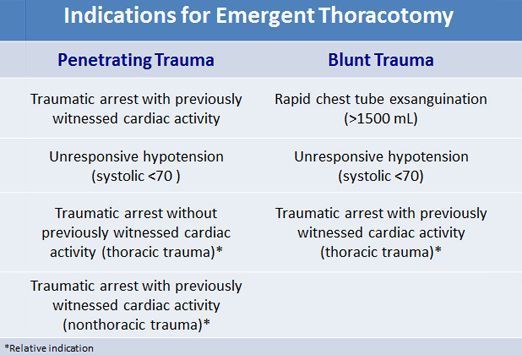 A left-sided approach is made in all traumatic arrests. With the patient supine and with several towels beneath the left scapula, raise the patient’s left arm above the head and secure it the elevated position. Prep the patient’s anterior chest bilaterally with iodine. In the anterolateral thoracotomy approach, an incision is made in the fourth intercostal space, starting at the sternum and extending to the posterior axillary line (shown). The initial incision should be deep enough to partially transect the latissimus dorsi muscle. Separate the skin, subcutaneous fat, and superficial portions of the pectoralis and serratus muscles with a no. 20 scalpel blade. Image courtesy of Wikimedia Commons. 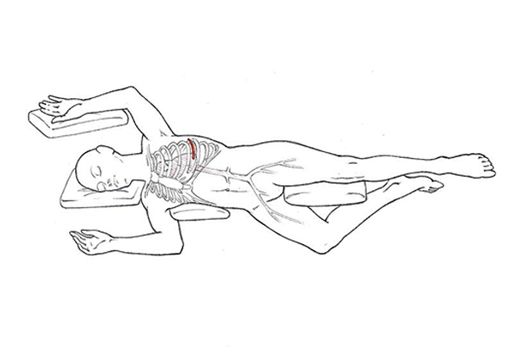 Stop ventilation momentarily just before entering the pleural cavity to collapse the lung and minimize iatrogenic injury. Make a small incision through the intercostal muscles. Place one blade of blunt-ended scissors into the hole, then completely transect the intercostal muscles. The operator may insert the fourth and fifth fingers of the free hand into the intercostal space and gently push away the lung to prevent injury. After transection of the intercostal muscles, place a rib spreader between the ribs to expose the intrathoracic contents (shown). Upon visualization of the thoracic cavity, use suction to evacuate clots and blood. Image courtesy of Cothren and Moore. 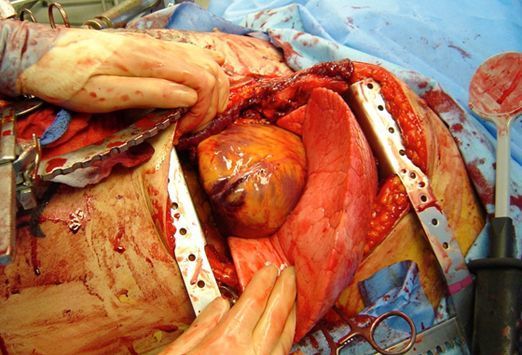 If injury to the right side of the heart is suspected, another incision can be made on the right, creating what is known as a clamshell (bilateral anterolateral thoracotomy) (shown). Alternatively, the sternum can be divided with trauma shears or a Gigli saw to extend the thoracotomy across the midline (called a trap door). Transection of the internal mammary arteries by this technique may result in significant bleeding once blood flow is restored. Image courtesy of the Journal of the Royal Army Medical Corps.  If the visualized thoracic contents do not reveal any obvious injury but cardiac injury is suspected, the pericardium must be opened. Enter the pericardium anterior to the phrenic nerve and just superior to the diaphragm to avoid injury to the great vessels. Use tissue forceps to grasp the pericardium and then incise the pericardium with scissors. Keep the point of the scissors parallel to the heart to prevent myocardium damage when extending the incision. After the initial incision, the operator may bluntly dissect the pericardium with fingers to avoid phrenic nerve laceration. The heart should be delivered from the pericardial sack and inspected for injury. Image courtesy of Wikimedia Commons.  Internal cardiac massage is performed with a two-handed technique; it can improve coronary perfusion pressure and increase return of spontaneous circulation with equal benefit in penetrating and blunt trauma. Internal defibrillator paddles and a chest tube may also be needed during EDT. Standard CPR delivers up to 20% of the cardiac output, whereas internal CPR produces up to 55% of the body's baseline perfusion.[7,8,9] This image shows internal paddles for defibrillation positioned on the anterior and posterior aspects of the heart. Start internal defibrillation at 20 J and increase to 40-50 J. Avoid touching the coronary arteries with the paddles. Image courtesy of Cothren and Moore. 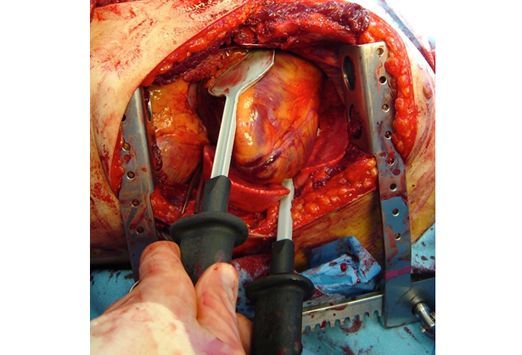 This image shows an aortic crossclamp (arrow) applied with the left lung retracted superiorly, below the inferior pulmonary ligament, just above the diaphragm. Cross-clamping the descending aorta redistributes the available blood flow to the coronary and cerebral arteries. Selective clamping of the descending aorta near the level of the diaphragm can also be used to control hemorrhage in abdominal vascular injuries. Clamping distally is ideal because it maximizes spinal cord perfusion and because the aorta is relatively mobile at this location. The flaccid aorta is identified as the first structure encountered on top of the spine when approached from the left chest. Image courtesy of Cothren and Moore. 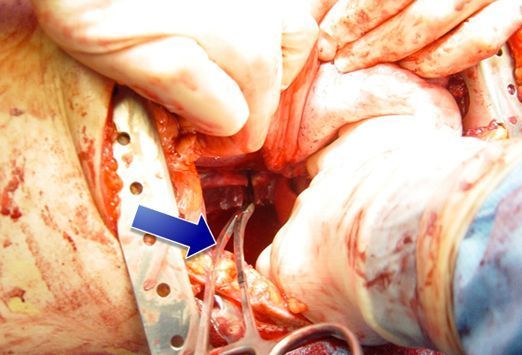 This patient arrived to the ED with a weak pulse and a systolic blood pressure of 40 mm Hg. He promptly died on the ED stretcher. An ED thoracotomy was performed for cardiopulmonary-cerebral resuscitation, and the aorta was cross-clamped. Note the proper positioning of the ratchet mechanism of the rib spreader to allow extension of the incision to the right chest for a clamshell thoracotomy if needed. 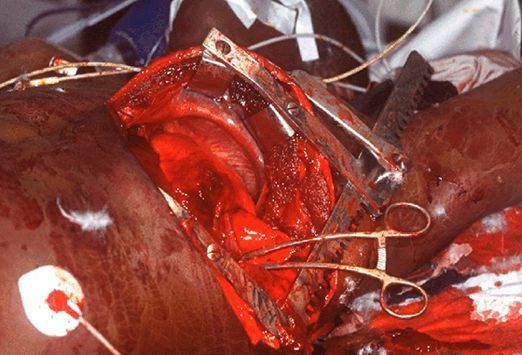 This chest radiograph shows a large right hemothorax, with endotracheal tube and tube thoracostomy. ED thoracotomy may be indicated for patients with massive hemothorax and imminent cardiac arrest. Generally, thoracotomy is required less than 15% of the time for these patients, with thoracostomy tube being the usual treatment for hemothoraces. Autotransfusion of evacuated blood can be an excellent adjunct for resuscitating these patients, particularly those in hemorrhagic shock. Image courtesy of the Journal of the Royal Army Medical Corps.  This patient was stabbed in the right chest with a knife. He presented to the emergency department (ED) short of breath and diaphoretic. His blood pressure was 105/77 mmHg, respiratory rate was 24, and his pulse was 100. His oxygenation on room air was 94%. Chest tube output was 100 cc/hour for 7 hours. A thoracotomy was performed.  Bleeding after a knife wound to the chest (shown) will stop spontaneously in the majority of cases and can be managed with a chest tube. In cases of traumatic hemothorax, surgical exploration should be performed if the patient experiences evacuation of more than 1 L of blood immediately after tube thoracostomy, has continued bleeding from the chest (150-200 mL/h for 2-4 hours), or requires repeated blood transfusions to maintain hemodynamic stability. Late sequelae of hemothorax (eg, residual clot, infected collections, trapped lung) require additional treatment, often including surgical intervention. 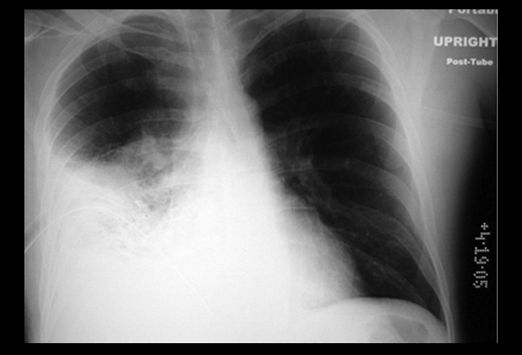 This alcoholic 50-year-old male patient with a history of schizophrenia sustained stab wounds into both ventricles and left lung, and survived following an emergency department thoracotomy. The EDT wound, however, became infected requiring serial debridements of soft tissue, rib cartilage, and sternum. This image shows the thoracotomy wound after a serial debridement of soft tissue, rib cartilage and bone, and the sternum. Image courtesy of Gilman et al.  |
|
#5
●
07-05-2012, 04:44 PM
| ||||||||
| ♚ Legacy Gold Member ♚ Poster Rank:35 Join Date: Mar 2012 Posts: 43,070
Contributions: 1
Mentioned: 251 Post(s) Quoted: 19389 Post(s)
| ||||||||
|
Re: Emergency Bedside Thoracotomy
Damn! That's a lot of shit to go through after the thoracotomy. He's schizo he probably doesn't even realize what happened.
|
|
#7
●
07-06-2012, 12:59 AM
| ||||||||
| ★ PSYCHOPOMP ★ Poster Rank:104 Man Join Date: Oct 2009 Posts: 15,927 Mentioned: 9 Post(s) Quoted: 1294 Post(s)
| ||||||||
|
Re: Emergency Bedside Thoracotomy
Wow that's some hard core butchering there. But when push comes to shove... the alternatives are bleak |























{kind=link}