|
#1
●
03-21-2012, 10:31 PM
| ||||||||
| ★ ********* ★ Poster Rank:247 Male Join Date: Jul 2009 Posts: 5,565
Contributions: 368
Mentioned: 66 Post(s) Quoted: 932 Post(s)
| ||||||||
|
Gunshot Wound Deaths
 An X-ray showing a partially fragmented bullet.  Breakup of a bullet in the neck on X-ray.  Breakup of a bullet within the cranial cavity as seen on X-ray.  An X-ray of a single intact 0.22 caliber bullet in the head in a suicide victim.  An X-ray showing the presence of two projectiles in the pelvis.  A gunshot entrance wound. Note the central round defect (hole) and the surrounding marginal abrasion. There is no surrounding soot or gunpowder stippling, making this a distant (indeterminate) range entrance wound. Note that the marginal abrasion is wider on the left side, indicating that the bullet was coming more from the left, as opposed to straight-on.  An example of an angled gunshot entrance wound. The bullet entered the skin at an angle, with initial contact at approximately the 11 o’clock position, traveling downward and slightly to the right as viewed in the photo.  An atypical gunshot entrance wound, characterized by a large size and relatively broad marginal abrasions. Such a wound typically occurs when the bullet has passed through an interposed target prior to striking the victim.  A bullet has entered and exited the arm and then reentered the left side of the thorax/back.  Fragmented bullet entrance wounds. If a bullet strikes an object prior to hitting a person, the bullet can fragment. Many times, the fragments maintain enough energy to enter the body.  An entrance wound of the thick (palmar) skin on the side of the hand. Note the presence of rare gunpowder stipple marks.  An entrance wound of the thick skin on the sole of a foot. Entrance wounds on the thick skin of the palms and soles often have an appearance that mimics an exit wound, lacking the typical circumferential marginal abrasion that most entrance wounds demonstrate.  Contact entrance wound of the scalp (forehead), showing the characteristic stellate shape due to splitting of the skin because of gases having dissected between the skin and underlying skull bones. Note the central round defect, as well as the soot.  A contact entrance wound of the head (forehead) showing wide separation of the wound edges. 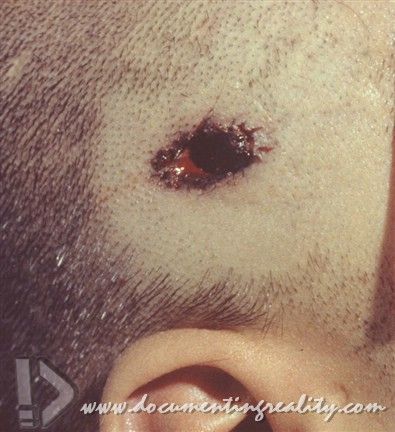 Not all contact wounds of the head have classic, large, stellate lacerations. This image shows a contact 0.22 caliber gunshot wound of the head (temple). Note the presence of soot, but the absence of significant stellate lacerations.  Loose contact wound of the chest, with extensive soot deposited around the entrance site.  (Left) A contact entrance wound of the scalp, with a muzzle imprint abrasion. The explosive gases force the surrounding skin against the muzzle of the weapon, resulting in the imprint abrasion. (Right) A view of the muzzle of the weapon used in this case. 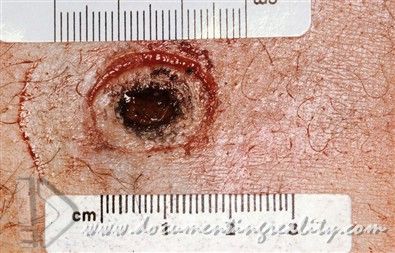 A contact gunshot wound of the chest with a surrounding muzzle impression.  A contact gunshot wound of the neck. Note the surrounding subcutaneous bleeding (blue discoloration. 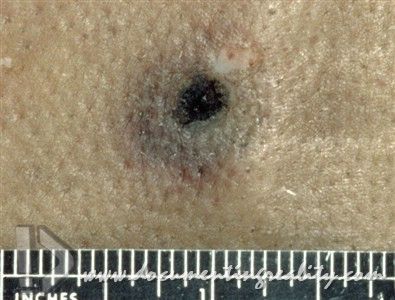 Contact gunshot wound of the chest.  Contact wound of the chest, with associated pink-red discoloration surrounding the wound, caused by the high carbon monoxide levels contained within the explosive gases of the gunshot discharge.  A characteristic site for suicide – a contact 0.22 caliber gunshot wound to the right temple with bruising of the soft tissues of the orbits.  Another characteristic site for suicide – a contact 0.22 caliber gunshot wound to the center of the forehead.  Soot soiling of the roof of the mouth in a suicide. Intraoral gunshot wounds are also a favored entrance site in suicides.  An intraoral gunshot wound of the roof of the mouth viewed via a mirror that has been inserted into the open mouth. Note the muzzle imprint and soot deposition.  Multiple lip lacerations associated with an intraoral suicidal gunshot wound.  A close-range gunshot wound, characterized by soot and gunpowder deposition. Such wounds typically occur when the muzzle of the weapon is within about 1 ft (12 in.) of the skin surface.  A close-range gunshot entrance wound with soot and stippling. 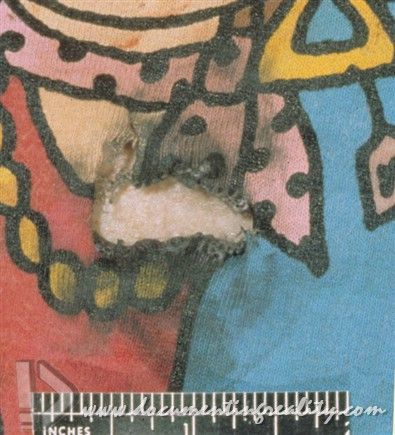 An article of clothing demonstrating soot deposition. It is important to examine the clothing of persons who have sustained gunshot injuries. In this case, the defect in the clothing has been moved away from the underlying gunshot wound in order to better visualize the soot.  An article of clothing with gunpowder deposition.  A medium (intermediate) range gunshot wound, characterized by gunpowder stippling, but no soot. These wounds typically occur when the muzzle of the weapon is from 1 to about 3 ft from the skin surface.  A medium (intermediate) range gunshot entrance wound with surrounding stippling.  Symmetrical stippling around an intermediate gunshot wound to the right side of the chest in a homicide. The symmetric pattern indicates that the bullet entered from a relative ‘‘straight-on’’ direction.  Symmetrical stippling around an intermediate homicidal gunshot wound to the left side of the chin.  Elliptical tattooing around an intermediate 0.45 caliber gunshot wound to the left chest, indicating an oblique angle of entrance.  Another angled entrance wound with more dense stippling on the skin closest to the gun (toward the right), and less dense stippling away from the gun (lower left). Note that the stippling extends a greater distance on the side opposite the gun.  A medium-range gunshot wound, where much of the gunpowder stippling has been blocked by hair on the upper right side of the image (it has been shaved at autopsy).  A gunshot entrance wound with surrounding stipple marks produced by fragments of an interposed target. Note the atypical appearance of the entrance wound, characteristic of a wound caused by a projectile that has gone through another object prior to hitting the body.  Dark discoloration of the margins of an entrance wound caused by postmortem drying. This can be misinterpreted as soot.  A stellate exit wound. Note the absence of a central round defect (a feature which is characteristic of an entrance wound). Exit wounds tend to be of irregular shape. They may or may not have a central round defect, and they usually lack circumferential marginal abrasions.  An irregularly shaped exit wound. Note the absence of marginal abrasions. 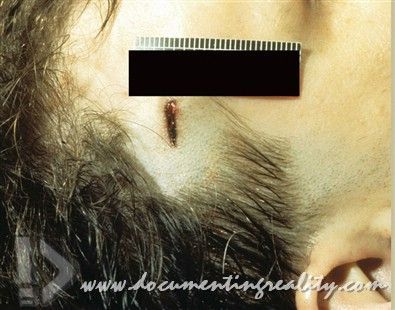 A slit-like gunshot exit wound.  An angled gunshot entrance wound (left) adjacent to an unrelated gunshot exit wound (right). Note that, although the exit wound has a central round- to oval-shaped defect, it lacks a marginal abrasion. 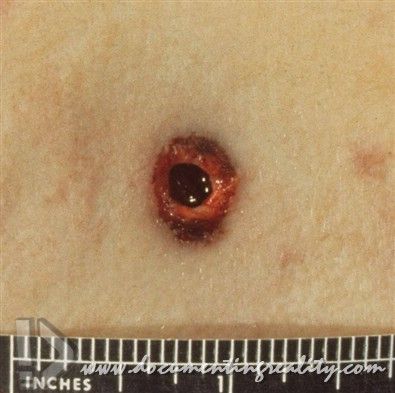 A shored exit wound where the decedent had been leaning against a supporting surface at the site of the exit wound. This prevents the typical irregular lacerations and mimics an entrance wound because the wound contains a circumferential marginal abrasion. 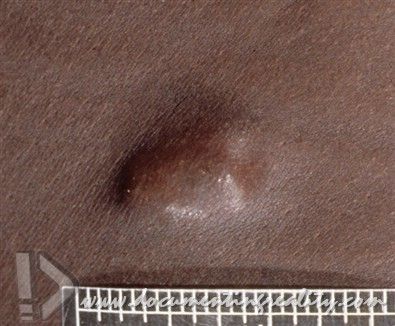 A bullet located just beneath the skin surface. 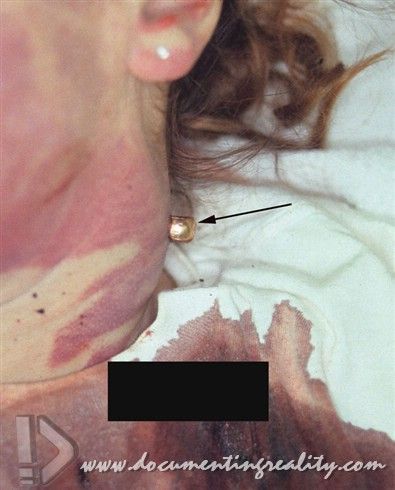 A partial gunshot exit wound of the neck, where the copper-jacketed bullet protrudes through the skin (arrow).  An area of subcutaneous hemorrhage indicating the location of a subcutaneous bullet.  A graze gunshot wound. The direction of bullet travel was from left to right. Note that the tips (pointed ends) of the skin ‘‘flaps’’ on the margins (upper and lower edges) point toward the gun.  Graze gunshot wound with the direction of travel of the bullet from right to left. 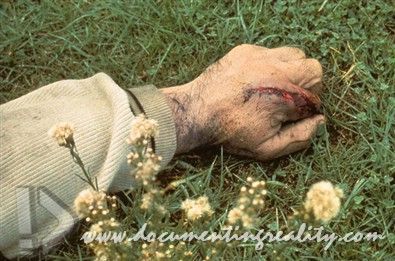 A graze wound of the hand from a 7.65 mm automatic.  An L-shaped cylinder-barrel gap mark, produced by gunshot residue being expelled from the cylinder barrel gap of a revolver.  An injury to the hand of a shooter caused by the slide of a semiautomatic pistol.  A high-velocity entrance wound. Note the relative absence of a marginal abrasion and the presence of numerous marginal microlacerations.  A distant-range, high-velocity entrance wound of the scalp with relatively extensive marginal lacerations.  High-velocity exit wounds, with extensive tissue damage.  A high-velocity rifle wound injury complex of the legs. The small entrance wound is just visible on the outside edge of the right thigh (left side of photograph – marked with an arrowhead). The large exit wound involves the inner aspect of the right thigh. Finally, there are multiple reentrance wounds from bullet fragments located on the inner aspect of the left thigh.  A close view of a high-velocity exit wound.  A suicidal contact high-velocity rifle wound of the chin, with a massive exit wound complex of the left side of the face.  A contact high-velocity entrance wound of the chest.  A contact shotgun wound of the forehead, with massive destruction.  Destruction of most of the head from a contact shotgun wound. 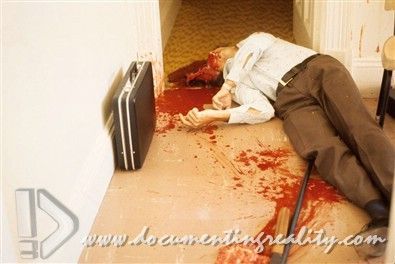 Destruction of most of the head from a contact shotgun wound with preservation of the avulsed brain (next to the shotgun in the foreground).  A contact shotgun wound of the lower chin. Note the stretch-type lacerations of the right side of the face.  Lacerations of the corners of the mouth and stretchtype lacerations of the cheek, related to a contact shotgun wound of the lower chin.  A contact shotgun wound of the chest. References Byard RW, Haas E, Marshall DT, Gilbert JD, Krous HF. Characteristic features of pediatric firearm fatalities – comparisons between Australia and the United States. J Forensic Sci. 2009;54:1093–6. Cina SJ, Ward ME, Hopkins MA, Nichols CA. Multifactorial analysis of firearm wounds to the head with attention to anatomic location. Am J Forensic Med Pathol. 1999;20:109–15. Clark MA, Micik W. Confusing wounds of entrance and exit with an unusual weapon. Am J Forensic Med Pathol. 1984;5:75–8. Cunliffe CH, Denton JS. An atypical gunshot wound from a home-made zip gun – the value of a thorough scene investigation. J Forensic Sci. 2008;53:216–8. DiMaio VJM. Gunshot wounds. 2nd ed. Boca Raton: CRC Press; 1999. Dodd MJ. Terminal ballistics – a text and atlas of gunshot wounds. Boca Raton: Taylor & Francis; 2006. Hartwig S, Tsokos M, Byard RW. Black powder handgun deaths remain anuncommon event. Am J Forensic Med Pathol. 2009;30:350–3. Hartwig S, Tsokos M, Schmidt S, Byard RW. Self-constructed shooting devices utilizing direct-impact firing pins – (suicide machines). Am J Forensic Med Pathol. 2010;31:192–4. Jacob B, Huckenbeck W, Daldrup T, Haarhoff K, Bonte W. Suicides by starter’s pistols and air guns. Am J Forensic Med Pathol. 1990;11:285–90. Juvin B, Brion F, Teissiere F, Durigon M. Prolonged activity after an ultimately fatal gunshot wound to the heart: case report. Am J Forensic Med Pathol. 1999;20:10–2. Karger B, Kneubuehl BP. On the physics of momentum in ballistics: can the human body be displaced or knocked down by a small arms projectile? Int J Leg Med. 1996;109:147–9. Kury G, Weiner J, Duval JV. Multiple self-inflicted gunshot wounds to the head: report of a case and review of the literature. Am J Forensic Med Pathol. 2000;21:32–5. Molina DK, Wood LE, DiMaio VJM. Shotgun wounds: a review of range and location as pertaining to manner of death. Am J Forensic Med Pathol. |
|
#3
●
03-21-2012, 10:48 PM
| ||||||||
| My Rank: LANCE CORPORAL Poster Rank:3475 male Join Date: Dec 2011 Posts: 101 Mentioned: 0 Post(s) Quoted: 1 Post(s)
| ||||||||
|
Re: Gunshot Wound Deaths
this is one of the best threads i've seen on this site
|
|
#6
●
03-22-2012, 09:15 AM
| ||||||||
| ✝Mudderator from Hell✝ Poster Rank:11 e-mail Join Date: Oct 2006 Posts: 95,376
Contributions: 817
Mentioned: 473 Post(s) Quoted: 10152 Post(s)
| ||||||||
|
Re: Gunshot Wound Deaths
Great info too. |
|
#10
●
03-22-2012, 12:07 PM
| ||||||||
| My Rank: MASTER SERGEANT Poster Rank:536 Male Join Date: Jan 2012 Posts: 1,886 Mentioned: 0 Post(s) Quoted: 22 Post(s)
| ||||||||
|
Re: Gunshot Wound Deaths
Great photos! You gotta love a shotgun for it's simplicity and devastation (not to mention not needing a perfect shot to do damage)
|


























{kind=link}