|
#1
●
03-18-2012, 07:53 AM
| ||||||||
| ★ ********* ★ Poster Rank:247 Male Join Date: Jul 2009 Posts: 5,565
Contributions: 368
Mentioned: 66 Post(s) Quoted: 932 Post(s)
| ||||||||
|
Asphyxial Deaths
While the term ‘‘asphyxia’’ literally means ‘‘without a pulse,’’ modern usage limits its application to cases where the body has been exposed to a significant reduction in oxygen levels resulting in impaired tissue oxygenation (delivery of oxygen to the body’s cells). It can result in reduced levels of oxygen (hypoxia), or absence of oxygen (anoxia). Unfortunately, there are no postmortem laboratory tests that can be performed to make a diagnosis of asphyxia as all bodies deoxygenate after death. If asphyxia is considered pathophysiologically, there are four stages where the transfer of oxygen can be compromised; i.e., oxygen reduction at the cellular level may be caused by (1) decreased amounts of oxygen in the environment, (2) reduced transfer from the air to the blood, (3) reduced transport from the lungs to the tissues, and (4) reduced transfer across cell membranes  Fig. 1 Petechiae represent multiple pinpoint areas of bleeding due to rupture of congested blood vessels. They are not specific for asphyxia, but are frequently present in certain types of death such as low suspension hanging where there has been compression of blood vessels. Typically, they occur over the eyelids  Fig.2 Conjunctival petechiae in a case of low suspension hanging. In full suspension hanging, petechaie are usually absent as pressure on neck vessels prevents congestion of the face  Fig.3 Petechiae of the eyelids in a case of low suspension hanging  Fig.4 Petechiae within the mouth in an asphyxial death  Fig.5 Laryngeal petechiae occurring in an asphyxial death  Fig.6 Petechiae may occur in a wide variety of situations, for example inside the lower eyelid in a death due to heart disease  Fig.7 A case of ‘‘simple’’ asphyxia (lack of environmental oxygen) with external airway obstruction by a plastic bag, in a suicidal drug overdose  Fig.8 A complex suicide utilizing a plastic bag over the head in addition to hanging  Fig.9 Injuries of the inner aspect of the lower lip in a smothering death where pressure was applied to the mouth and nose 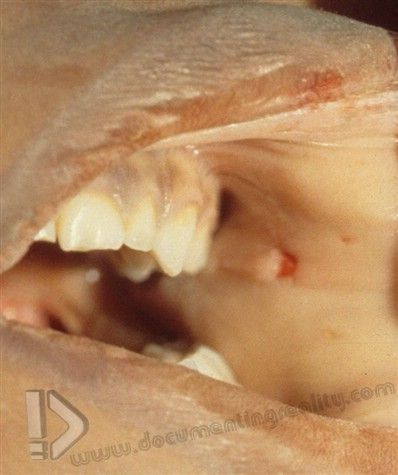 Fig.10 Injuries to the inner cheek in a homicidal smothering case  Fig.11 Obstruction of the inner airway by food is one of the most common causes of choking deaths. In this case, impacted food completely occludes the larynx. Accidental choking on food or so-called ‘‘cafe´ coronary’’ occurs in demented individual with poor dentition or in association with intoxication  Fig.12 A choking death in an intoxicated individual, with occlusion of the larynx and upper trachea by a large fragment of meat 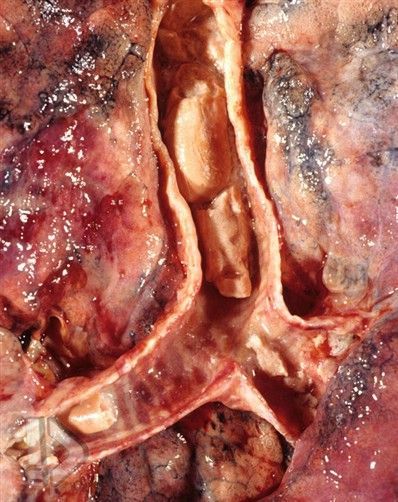 Fig.13 A choking death due to lower airway obstruction by multiple pieces of hot dog, evident within the trachea and mainstem bronchi. Rounded foods such as portions of sausage, carrots, and grapes are often implicated in such deaths 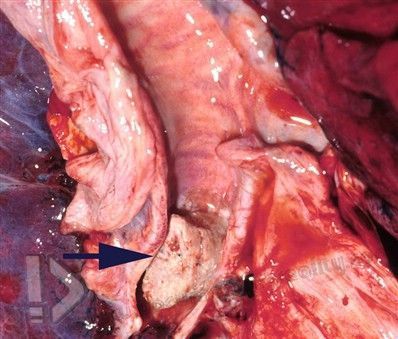 Fig.14 A single portion of unchewed sausage wedged into a main bronchus (arrow) may be sufficient to cause death  Fig.15 In the case shown, choking had occurred on scrambled eggs which can be seen draining out of the mouth 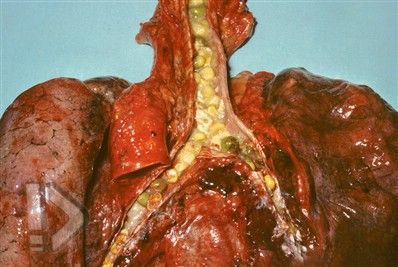 Fig.16 Complete filling of the major airways with inhaled vegetable matter 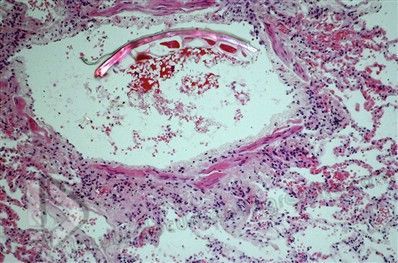 Fig.17 Microscopy may reveal inhaled material in the smaller airways. A piece of vegetable matter in a bronchiole is highlighted by polarizing  Fig.18 An edematous (swollen) epiglottis and inlet to the larynx in a death related to anaphylaxis (allergic reaction) 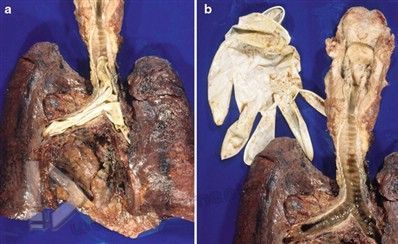 Fig.19 Internal airway obstruction with a latex examination glove (a) that has been removed at autopsy (b)  Fig.20 An asphyxial death due to underlying natural disease in a decomposed body. Note the tumor occluding the laryngeal opening. Although the tumor is a benign tumor of fat tissue (a ‘‘lipoma’’), it was lethal because of its location  Fig.21 Blockage of the upper airway due to tonsillar enlargement from infectious mononucleosis (glandular fever), an infection that causes enlargement of the tonsils, lymph nodes, and spleen. The top of the tongue is seen in the lower portion of the photo 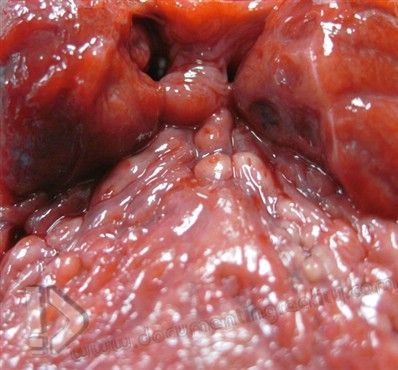 Fig.22 Marked narrowing of the airway at the back of the tongue due to tonsillitis. The uvula can be seen in the center of the field touching the two enlarged tonsils 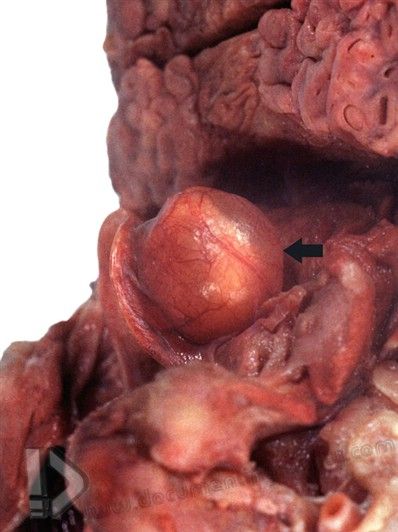 Fig.23 Other natural causes of acute upper airway obstruction include cysts of the back of the tongue or the epiglottis (arrow) as illustrated 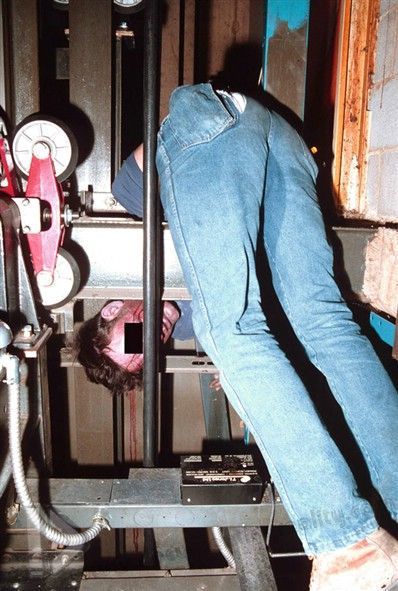 Fig.24 A case of traumatic asphyxia in which a worker became pinned between an I-beam and a descending elevator as he was leaning into the elevator shaft  Fig.25 Petechiae of the inner eyelid in a case of traumatic compression when a man became pinned underneath an overturned tractor  Fig.26 Chest injuries occurring in a man who was working under a mobile home when it fell off of its supports and crushed him. Other than florid facial petechiae, the only other injuries present at autopsy were the external chest injuries depicted here, that are in keeping with the history of being compressed 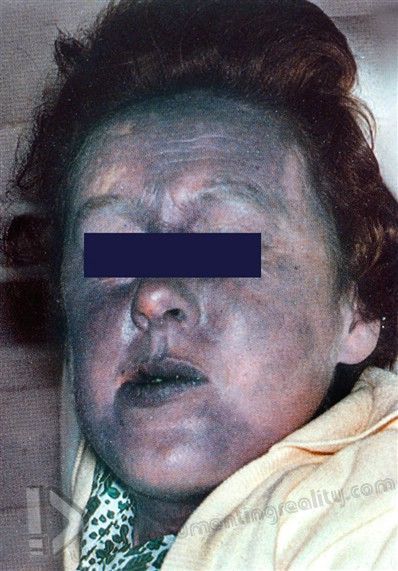 Fig.27 Intense congestion of the face also occurs in crush asphyxia  Fig.28 In addition to facial congestion and petechiae, there may be marked conjunctival congestion and hemorrhage in crush asphyxia  Fig.29 Intense petechiae are usually found in the skin of the face, neck, and upper trunk in cases of crush asphyxia, except in areaswhere capillaries are compressed by tight-fitting clothing, such as under a brassiere  Fig.30 Extensive posterior neck muscle hemorrhage identified in a motor vehicle collision-related traumatic asphyxial death 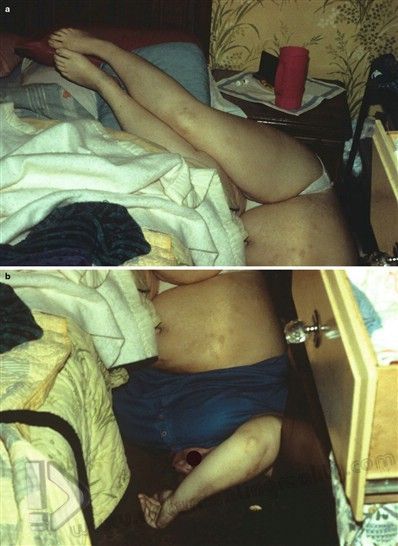 Fig.31 (a, b) Positional asphyxia related to acute ethanol intoxication. Note the fact that the body is essentially ‘‘upside down’’ and the neck is markedly kinked  Fig.32 Lower facial petechiae in an individual who died of positional asphyxia (upside down body position) in a rollover motor vehicle collision  Fig.33 Extensive facial petechiae of the eyelid and forehead in another case of positional asphyxia 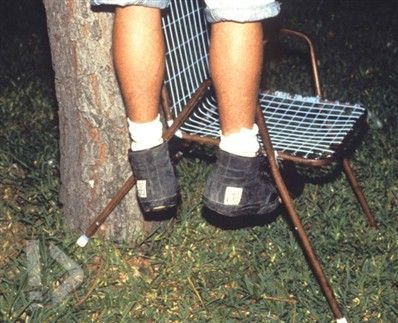 Fig.34 A full-suspension hanging death, with the feet totally off the ground. The chair enables the decedent to tie the rope to a high point  Fig.35 A partial-suspension hanging death, with the feet touching the ground  Fig.36 A low-suspension hanging death where the victim presumably used milk crates to stand on in order to attach the ligature to an overhead support  Fig.37 A hanging death with a rope used as a ligature 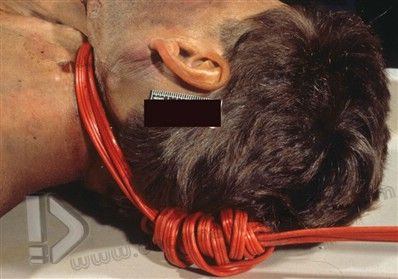 Fig.38 A hanging death in which an extension cord was used as the ligature 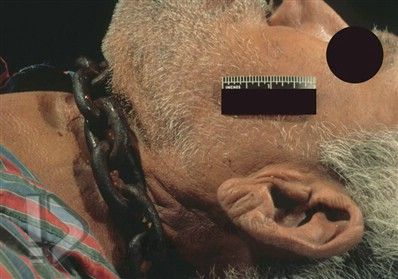 Fig.39 A suicidal hanging death utilizing a chain as the ligature 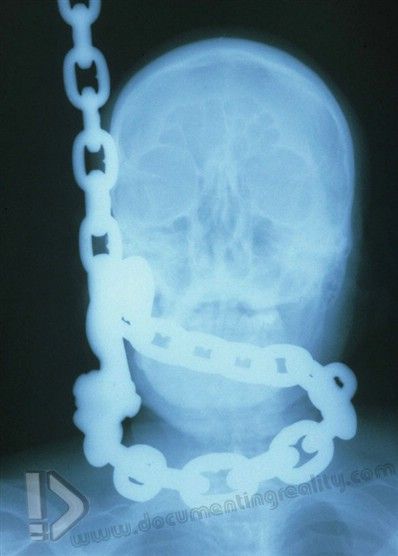 Fig.40 An x-ray of the case shown in >Fig. 39 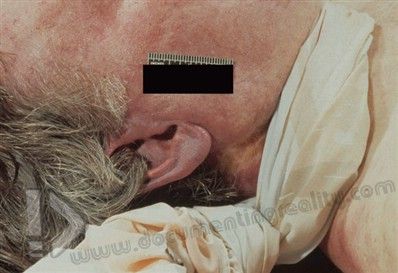 Fig.41 A suicidal hanging death utilizing a bed sheet as the ligature. Due to the broader area of the sheet compared to thin ropes, marks on the neck may be less obvious (see >Fig. 48)  Fig.42 A typical parchmented (dry) ‘‘furrow’’ mark is evident underlying the ligature. Note that it takes on the shape of the braided rope which was used as the ligature and angles sharply upward to the point of suspension  Fig.43 Nylon dog leads are often used as ligatures in suicidal hangings Fig.44  Removal of the lead in the case illustrated in >Fig. 43 reveals a distinct weave pattern marking the skin that corresponds exactly to the weave of the ligature. The ligature and parchmented weave pattern around the neck should be photographed together to document the concordance  Fig.45 A looped nylon rope around the neck in a suicidal hanging 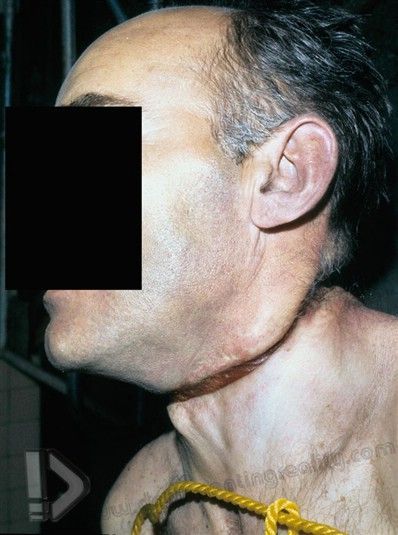 Fig.46 A typical parchmented mark underneath the ligature in >Fig. 45  Fig.47 An obvious furrow mark caused by coaxial cable in a suicidal hanging death 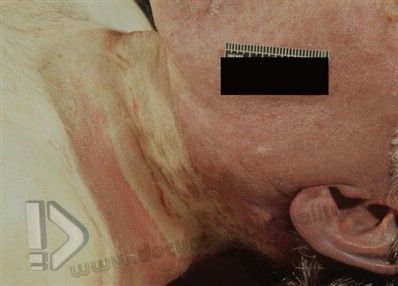 Fig.48 A less obvious furrow mark produced by a bed sheet (see >Fig. 41)  Fig.49 Suicidal hanging differs from homicidal ligature strangulation as the loop around the neck in suicide rises to the point of suspension, as is very clearly shown here  Fig.50 When the ligature is removed in a suicidal hanging, a ‘‘V’’ shaped furrow can usually be seen. In homicidal ligature strangulation, the furrow from the ligature is more horizontal 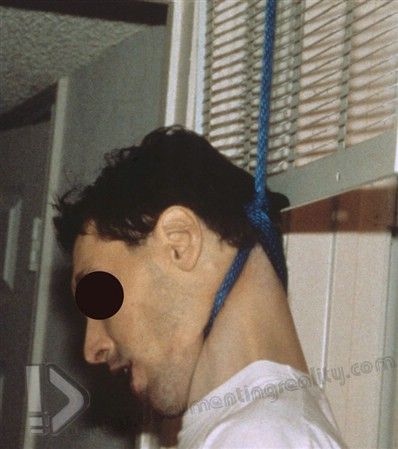 Fig.51 Again a marked upward angle of the rope along the left side of this suicide victim’s neck and head  Fig.52 A ligature furrow mark on the posterior aspect of a suicidal hanging victim’s neck, with upward angulation (inverted ‘‘V’’ shape) 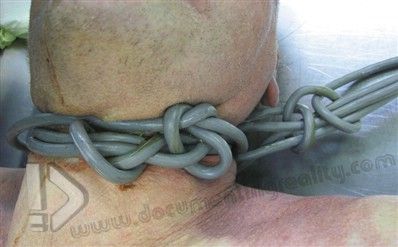 Fig.53 Knots in suicidal hanging may be very complex, as can be seen in this case in which an electric flex was used  Fig.54 A typical furrow may have a ‘‘tram track’’ appearance with central pallor and reddened edges  Fig.55 A double-looped ligature used in hanging will result in two underlying furrows  Fig.56 If a ligature slips during hanging, there may be two furrows. In the case illustrated, an alternative explanation for this injury pattern would be a ligature homicide (producing the lower horizontal furrow) disguised as a suicidal hanging (producing the upper angled furrow beneath the ear)  Fig.57 Tardieu spots on the leg of a hanging victim are produced by postmortem rupture of intensely congested small blood vessels  Fig.58 Fixed lividity with blanching on the sole of a hanging victim’s foot, indicating that the foot was in contact with the ground in a low-suspension hanging  Fig.59 As the structures of the neck, including the tongue, are lifted upward during hanging, the tip of the tongue often protrudes from the mouth and dries out, giving it a dark appearance 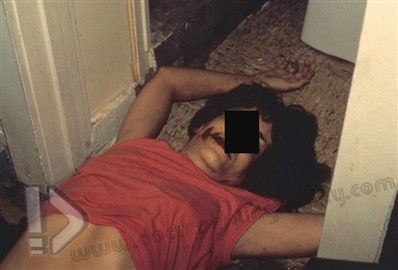 Fig.60 A strangulation death scene. Careful examination of the scene, the clothing, and the body may provide valuable evidence that could link a perpetrator to the crime  Fig.61 Irregular ligature marks in a homicidal strangulation case  Fig.62 A case of ligature strangulation, viewed from the side. Note the lack of upward angulation of the mark which distinguishes it from the usual ligature mark in suicidal hanging 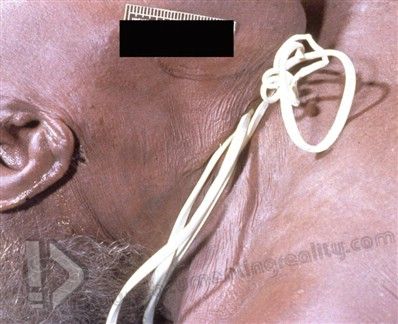 Fig.63 A telephone line cord used as a ligature in a homicidal strangulation case has been left in place by the assailant  Fig.64 A homicidal ligature strangulation case in which a ‘‘zip-tie’’ was used as a ligature. Unlike most strangulation cases, the internal neck examination in this case revealed no soft tissue hemorrhage  Fig.65 Extensive congestion of the skin with petechiae above the level of the ligature mark in a case of homicidal strangulation  Fig.66 A more subtle ligature furrow mark in a homicidal strangulation case, viewed from the back. Note that the mark is relatively horizontal and lacks the upward angulation that is typical of hanging furrow marks  Fig.67 Symmetrical abrasions of the side of the neck in a case of manual strangulation  Fig.68 Injuries to the neck in homicidal manual strangulation deaths may be quite subtle 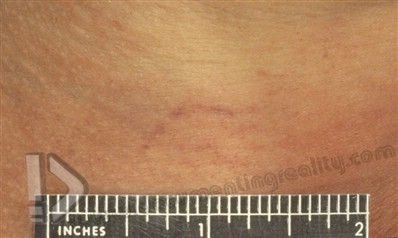 Fig.69 A close-up view of a fingernail scratch mark on the neck of the manual strangulation victim shown in >Fig. 68 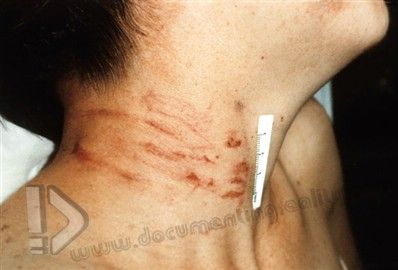 Fig.70 Scratch marks around the neck from manual strangulation where the perpetrator was standing behind the victim  Fig.71 Postmortem ant activity may cause lesions on the neck that can be mistaken for strangulation marks  Fig.72 Anterior neck ‘‘strap’’ muscle hemorrhage in a strangulation case 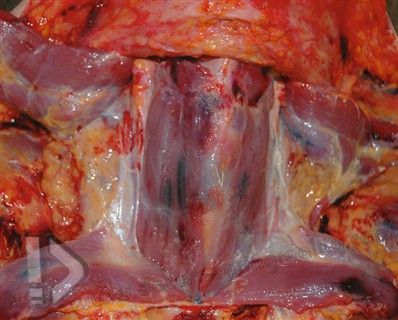 Fig.73 Multiple, relatively small areas of anterior neck strap muscle hemorrhage in a homicidal strangulation case 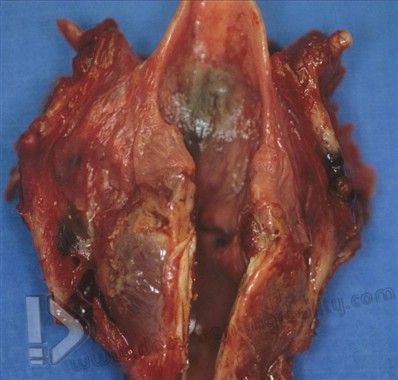 Fig.74 Multiple fractures of the laryngeal cartilages (with surrounding soft tissue hemorrhage), related to a homicidal strangulation 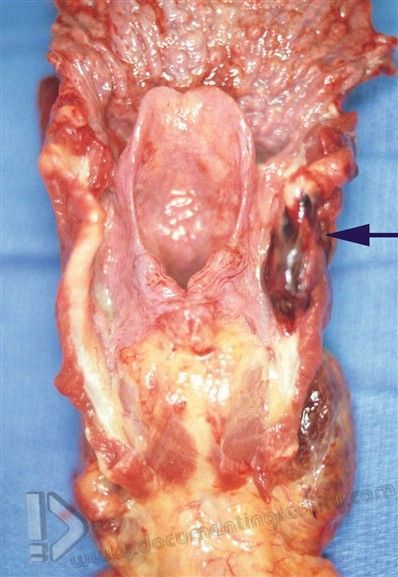 Fig.75 A localized fracture of the right horn of the thyroid cartilage in a homicidal strangulation case (arrow)  Fig.76 A lateral hyoid bone fracture caused by neck pressure during strangulation. Note the hemorrhagic soft tissue surrounding the site of the fracture (arrow), compared to the other side which was not injured  Fig.77 A fracture closer to the front of the hyoid bone in a case of ligature strangulation  Fig.78 Posterior neck hemorrhage demonstrated by postmortem dissection in a homicidal strangulation case  Fig.79 A scene photograph showing a woman who committed suicide by carbon monoxide/exhaust inhalation, a type of ‘‘chemical asphyxia,’’ as carbon monoxide binds to hemoglobin, preventing oxygenation of blood  Fig. 80 Interior view of the automobile used in the carbon monoxide suicide depicted in >Fig. 15.79 with the key in the ‘‘on’’ position  Fig.81 A scene photograph in a case of suicidal carbon monoxide inhalation in which the victim used a vacuum cleaner hose to blow exhaust into the interior of a car (Photo courtesy of Dr. Patrick E. Lantz, MD, Department of Pathology, Wake Forest University School of Medicine, Winston-Salem, NC)  Fig.82 Interior view of the case depicted in>Fig. 81 with a vacuum cleaner hose running from the exhaust to the cabin of the vehicle (Photo courtesy of Dr. Patrick Lantz, Department of Pathology, Wake Forest University School of Medicine, Winston-Salem, NC)  Fig.83 A vacuum cleaner hose connected to an exhaust pipe in a case of suicide in a car from inhaling exhaust fumes (Photo courtesy of Dr. Patrick Lantz, Department of Pathology, Wake Forest University School of Medicine, Winston-Salem, NC) 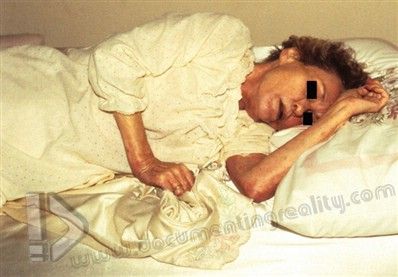 Fig.84 An elderly woman found dead in her bed. The previous day, her furnace had been professionally serviced. Toxicological analyses showed that she had lethal levels of carbon monoxide in her blood 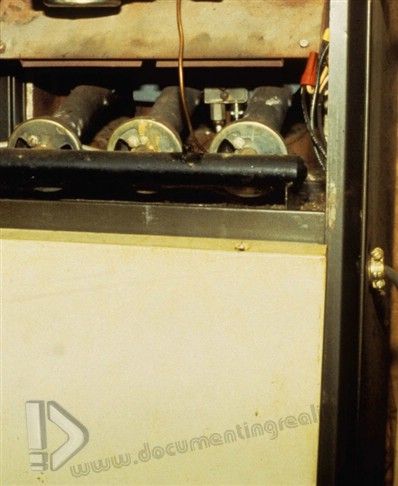 Fig.85 Examination of the furnace (see >Fig. 84) by an expert in the heating business revealed that it was not venting properly, resulting in carbon monoxide release into the home  Fig.86 Comparison of the color of lividity in a natural death (left) with a death from carbon monoxide inhalation (right) showing the brighter cherry red discoloration that occurs with carbon monoxide exposure (Photo courtesy of Dr. Patrick Lantz, MD Department of Pathology, Wake Forest University School of Medicine, Winston-Salem, NC) 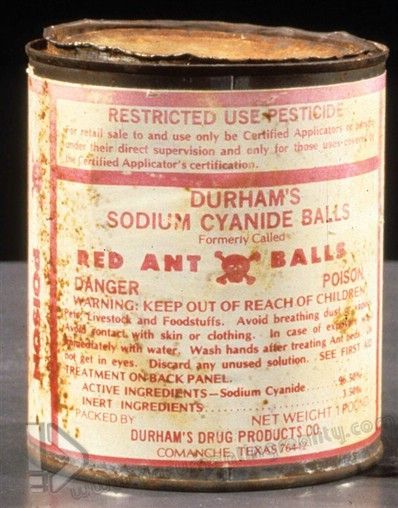 Fig.87 A container of cyanide used in a suicidal ingestion case (Courtesy of the Dallas County Medical Examiners Office, Jeffrey J. Barnard, Chief Medical Examiner) 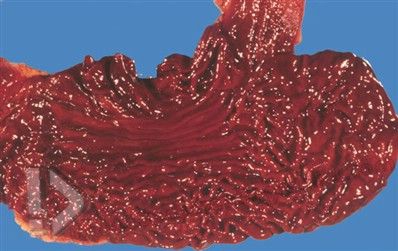 Fig.88 Gastric (stomach) mucosa hemorrhage in a case of cyanide poisoning (Courtesy of the Dallas County Medical Examiners Office, Jeffrey J. Barnard, Chief Medical Examiner) 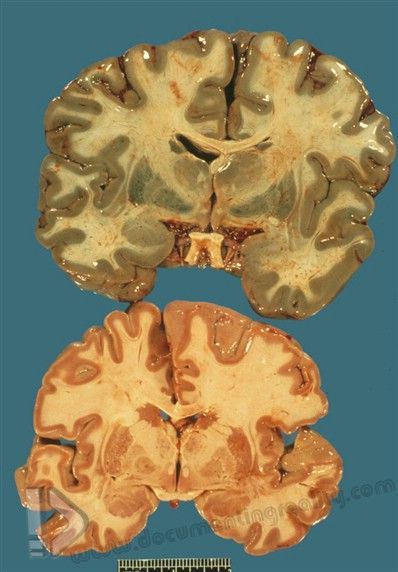 Fig.89 The brain of a man who died of hydrogen sulfide gas inhalation (above) compared to a brain from someone who died of natural causes (below) revealing the characteristic green discoloration from exposure to hydrogen sulfide (Courtesy of the Dallas County Medical Examiners Office, Jeffrey J. Barnard, Chief Medical Examiner) 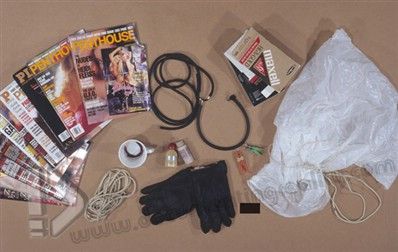 Fig.90 Pornographic and other items found at the scene of an autoerotic asphyxia death 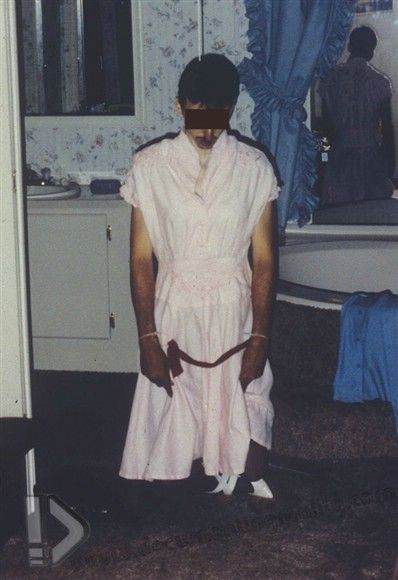 Fig.91 An autoerotic asphyxia death where the victim dressed in female clothing and loosely bound his hands  Fig.92 Underclothing worn by the autoerotic asphyxia victim depicted in >Fig. 91 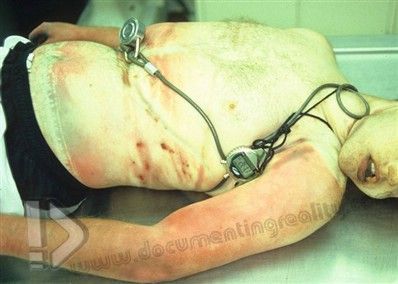 Fig.93 A cable wrapped about the body of a victim who died of accidental autoerotic asphyxia  . Fig.94 (a, b) An autoerotic asphyxial death in which the cross-dressed victim used duct tape, a variety of ligatures, and Freon gas  Fig.95 Female underclothing, ligatures, and handcuffs are not infrequently found in cases of autoerotic death  Fig.96 A closer view of the decedent’s legs in the case from >Fig. 95 showing binding with strips of panty hose and a set of cuffs 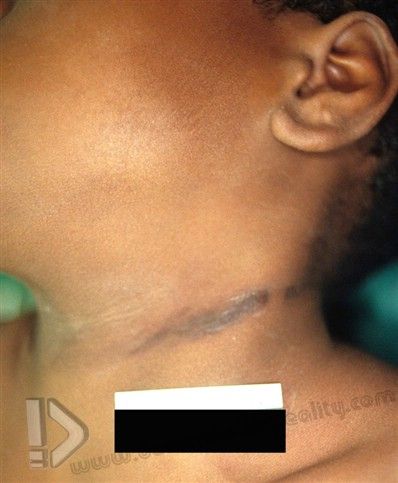 Fig.98 Restraint asphyxia death reenactment. Notice that the victim is face-down, with his hands cuffed behind his back, with multiple police officers applying force to his back 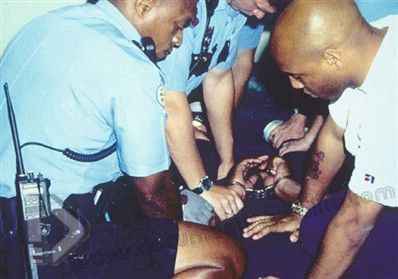 Fig.97 Ligature marks on the neck of a 9-year-old boy found partially suspended from a bandana looped about his neck, as a result of the ‘‘choking game’’ References Andrew TA, Fallon KK. Asphyxial games in children and adolescents. Am J Forensic Med Pathol. 2007;28:303–7. Azmak D. Asphyxial deaths – a retrospective study and review of the literature. Am J Forensic Med Pathol. 2006;27:134–44. Amanuel B, Byard RW. Accidental asphyxia in bed in severely disabled children.J Paediatr Child Health. 2000;36:66–8. Byard RW. The brassiere ‘‘sign’’ – a distinctive marker in crush asphyxia. J Clin Forensic Med. 2005a;12:316–9. Byard RW. Autoerotic death. In: Payne-James J, Byard RW, Corey T, Henderson C, editors. Encyclopedia of forensic and legal medicine, vol. 1. Amsterdam:Elsevier/Academic; 2005b. p. 157–65. Byard RW. Issues in the classification and pathological diagnosis of asphyxia. Aust J Forensic Sci. 2011;43:27–38. Byard RW, Bramwell NH. Autoerotic death. A definition. Am J Forensic Med Pathol. 1991;12:74–6. Byard RW, Charlwood C. Lethal head entrapment – a specific problem of early childhood. J Forensic Leg Med. 2009;16:340–2. Byard RW, Gilbert JD. Sleeping accidents in the elderly. J Forensic Sci. doi: 10.1111/j.1556-4029.2011.01838.x. Byard RW, Hanson KA, James RA. Fatal unintentional traumatic asphyxia in childhood. J Paediatr Child Health. 2003;39:31–2. Byard RW, Hanson K, James RA, Gilbert JD. Suicide methods in the elderly in South Australia 1981–2000. J Clin Forensic Med. 2004;11:71–4. Byard RW, Hucker SJ, Hazelwood RR. A comparison of typical death scene features in cases of fatal male and female autoerotic asphyxia with a review of the literature. Forensic Sci Int. 1990;48:113–21. Byard RW, Jensen L. Fatal asphyxial episodes in the very young – classification and diagnostic issues. Forensic Sci Med Pathol. 2007;3:177–81. Byard RW, Simpson E, Gilbert JD. Temporal trends over the past two decades in asphyxial deaths in South Australia involving plastic bags or wrapping. J Clin Forensic Med. 2006a;13:9–14. Byard RW, Tsokos M. Infant and early childhood asphyxial deaths – diagnostic issues. In: Tsokos M, editor. Forensic pathology reviews, vol. 2. Totowa: Humana Press; 2005. p. 101–23. Byard RW, Wick R, Gilbert JD. Conditions and circumstances predisposing to death from positional asphyxia in adults. J Forensic LegMed. 2008;15:415–9. Byard RW, Wick R, Simpson E, Gilbert JD. The pathological features and circumstances of death of lethal crush/traumatic asphyxia in adults – a 25-five year study. Forensic Sci Int. 2006b;159:200–5. Byard RW, Winskog C. Autoerotic death: incidence and age of victims – a population based study. J Forensic Sci. doi: 10.1111/j.1556-4029.2011.01898.x. Byard RW, Woodford N. Automobile door entrapment – a different form of vehicle-related crush asphyxia. J Forensic Leg Med. 2008;15:339–42. Carrick C, Collins KA, Lee CJ, Prahlow JA, Barnard JJ. Sudden death due to asphyxia by esophageal polyp: two case reports and review of asphyxial deaths. Am J Forensic Med Pathol. 2005;26(3):275–81. Combrinck M, Byard RW. Infant asphyxia, soft mattresses and the ‘‘trough’’ effect. Am J Forensic Med Pathol (in press) Conroy C, Eastman AB, Stanley C, Vilke GM, Vaughan T, Hoyt DB, Pacyna S. Fatal positional asphyxia associated with rollover crashes. Am J ForensicMed Pathol. 2007;28:330–2. Dix J, Graham M, Hanzlick R. Asphyxia and drowning – an atlas. Boca Raton: CRC Press; 2000. Ely SF, Hirsch CS. Asphyxial deaths and petechiae: a review. J Forensic Sci. 2000;45(6):1274–7. Focardi M, Gualco B, Norelli G. Accidental death in autoerotic maneuvers. Am J Forensic Med Pathol. 2008;29:64–8. Gilbert J, Jensen L, Byard RW. Further observations on the speed of death in hanging. J Forensic Sci. 2008;53:1204–5. Green H, James RA, Gilbert JD, Byard RW. Fractures of the hyoid bone and laryngeal cartilages in suicidal hanging. J Clin Forensic Med. 2000;7:123–6. Hashimoto Y, Moriya F, Furumiya J. Forensic aspects of complications resulting from cardiopulmonary resuscitation. Leg Med. 2007;9:94–9. James RA, Byard RW. Asphyxiation from shoulder seat belts. An unusual motor vehicle injury. Am J Forensic Med Pathol. 2001;22:193–19. Kojima T, Nishiyama Y, Yashiki M, Une I. Postmortem formation of carbon monoxide. Forensic Sci Int. 1982;19:243–8. Prahlow JA, Barnard JJ. Fatal anaphylaxis due to fire ant stings. Am J Forensic Med Pathol. 1998;19:137–42. Prahlow JA, Doyle BW. A suicide using a homemade carbon monoxide ‘‘death machine. Am J Forensic Med Pathol. 2005;26:177–80. Schon CA, Ketterer T. Asphyxial suicide by inhalation of helium inside a plastic bag. Am J Forensic Med Pathol. 2007;28:364–7. Shields LBE, Hunsaker DM, Hunsaker JC. Autoerotic asphyxia: part I. Am J Forensic Med Pathol. 2005;26:45–52. Wick R, Gilbert JD, Byard RW. Cafe´ coronary syndrome – fatal choking on food: an autopsy approach. J Clin Forensic Med. 2006;13:135–8. |
|
#2
●
03-18-2012, 08:09 AM
| ||||||||
| ★ Legacy Member ★ Poster Rank:133 meow Join Date: Nov 2011 Posts: 12,249
Contributions: 41
Mentioned: 11 Post(s) Quoted: 438 Post(s)
| ||||||||
|
Re: Asphyxial Deaths
Awesome post! My fave subject |
|
#8
●
03-18-2012, 11:41 AM
| ||||||||
| My Rank: FIRST SERGEANT Poster Rank:394 Join Date: Apr 2011 Posts: 3,054 Mentioned: 2 Post(s) Quoted: 276 Post(s)
| ||||||||
|
Re: Asphyxial Deaths
This is a real masterpiece of a post! You always seem to make such big an effort in bringing content here - maybe I should follow your example as well |


























{kind=link}