Urethro-vaginal fistulae (UVF) are rare in the developed world; they are usually caused by obstructed labour and birth trauma, surgical complications, malignancy and radiation therapy. We present a case of a UVF in a patient with a long term history of utero-vaginal prolapse. In the absence of any known causative factor in the case, we speculate that chronic pressure ulcers and vaginal atrophy associated with the procidencia caused the UVF. The patient was treated with vaginal hysterectomy, pelvic floor repair and UVF repair using a Martius flap, as a single procedure following which she has no more urinary incontinence.
Introduction
Urinary fistulae have significant physical, psychological and social impact on women’s health. The first successful fistula repair was reported in 1852 by J. Sims [1]. Urethro-vaginal fistulae (UVF), through common in developing areas, are rare in the developed world and are usually seen as a complication following treatment to the area. Spontaneously-arising (UVF) is very uncommon.
Case presentation
We report a case of a 72 year old Caucasian woman with procidencia who developed a UVF without an obvious prior cause. She presented with a history of intermittent urinary incontinence, difficulty in passing urine, and recurrent urinary tract infections (UTI’s) for over a year, on a background of a long term history of procidencia. Over the preceding 12 months she had 7 episodes of confirmed UTI, together with intermittent urinary incontinence. In the last episode of UTI, pseudomonas was isolated, and she required prolonged hospitalisation and intravenous gentamycin to recover. Following this episode, she was advised to see a gynaecologist. Her previous gynaecological history involved an uncomplicated normal vaginal delivery 40 years ago and she was menopausal for 21 years. She used hormonal replacement therapy for a short period; however after a cerebrovascular accident at the age of 57 she discontinued it. The stroke left her with left hemiplegia, hemisensory loss and wheelchair bound. Despite this, her bladder function remained satisfactory and she did not require catheterisation. Additionally, she was on treatment for hypertension for over 20 years (non-diuretic medication). Gynaecological examination in clinic was difficult due to her restricted mobility, but revealed a procidencia with ulceration and atrophy of the vaginal epithelium. A fistula was not immediately apparent; however the bladder was noted to be completely invaginated by the procidencia. Her symptoms were attributed to this and she was given the treatment options of a vaginal pessary or a vaginal hysterectomy with a pelvic floor repair after anaesthetic review. She was keen to try the pessary. A size 85mm, then a size 90mm pessary were fitted during the consultation, however, both fell out within 10 minutes of insertion and it was noticed that she had involuntary loss of urine when the procidencia was reduced. Following this, it was agreed to proceed to surgery. Her preoperative assessment included blood tests for haemoglobin and renal function, and urine culture. Her creatinine levels were noted to be abnormal at 138μmol/L when compared to levels of 80 μmol/L two years previously (normal range 58-96).
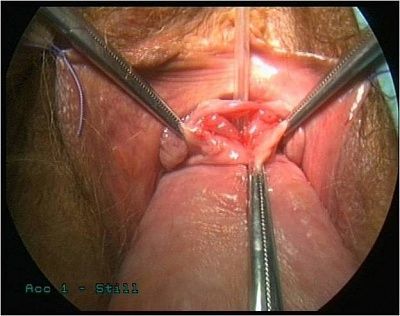
During initial examination under anaesthesia (EUA), procidencia with a low vaginal fistula of approximately 2 cm was identified.
Examination findings of procidencia with arrow showing a low vaginal fistula

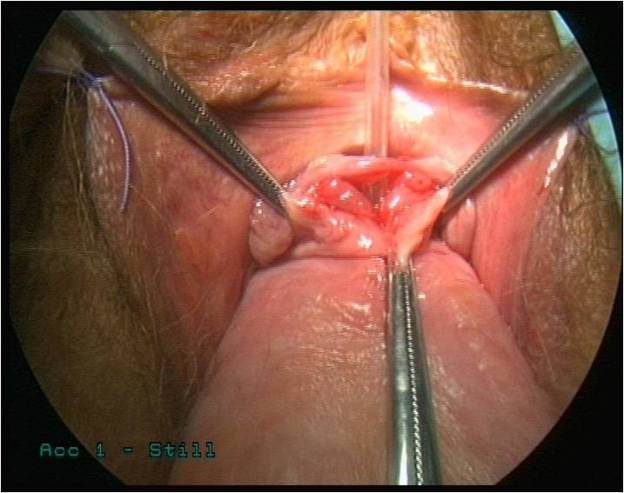
Identification of urethro-vaginal fistula

























{kind=link}