|
#1
●
07-13-2014, 07:42 PM
| ||||||||
| ✖ The Antique Christ ✖ Poster Rank:105 Gonzo Punk Join Date: Jan 2009 Posts: 15,488
Contributions: 58
Mentioned: 23 Post(s) Quoted: 2046 Post(s)
| ||||||||
|
Lucio's Phenomenon in Leprosy
Lucio's phenomenon is an unusual reaction seen almost exclusively in patients from the Caribbean and Mexico with diffuse, lepromatous leprosy, especially in untreated cases. It is characterised by recurrent crops of large, sharply demarcated, ulcerative lesions, affecting mainly the lower extremities, but may generalise and become fatal as a result of secondary bacterial infection and sepsis. Lucio's phenomenon was first described by Rafael Lucio Nájera and Alvarado as a necrotizing skin reaction associated with non-nodular diffuse leprosy in 1852. This reaction was later named by Latapi and Zamora in 1948 as Lucio's phenomenon after identification of histopathological changes involving multiple, acute and necrotizing cutaneous vasculitis peculiar to pure and primitive diffuse leprosy (PPDL). -------------------------------------------------------  Figure 1. Vasculitic ulcerated lesions over the pinna  Figure 2. Superficial angulated ulcers seen over the thighs and scrotum  Figure 3. Necrotizing lesions over the buttocks  Figure 4. Deep necrotic ulcers covered with yellow slough over lower legs A 65-year-old man from Tamilnadu was referred to us from the Department of Medicine with cutaneous ulcerations over the legs, hands, abdomen, buttocks and pinna, along with fever, arthralgia and anorexia for past 10 days. These ulcers had first appeared over bilateral lower legs as painless, scarlet spots of irregular bizarre shapes that later darken and ulcerate, leaving atrophic and hypochromic scars with a thin hyperpigmented border in some areas. Within 2 days, similar lesions appeared involving the trunk, upper limbs as well as pinna of both ears. He had been diagnosed as a case of leprosy 15 years before and advised to take anti-leprosy treatment but due to social stigma, he had refused to take any treatment in spite of being aware of his disease. He had experienced similar ulcerations mainly over his lower legs repeatedly for the last year which earlier used to heal spontaneously with antibiotics from a local doctor. However, this episode, being more severe, he was referred to our institute. No new ulcers appeared further and the ulcers started healing over the following 2 weeks but he developed MRSA (multidrug resistant Staphylococcus aureus) septicemia and died on the 16th day of hospitalization. -----------------------------------------------------  Figure 1. Clinical Photograph showing multiple plaques with ulcerations over abdomen, forearms and arm  Figure 2. Clinical photograph showing ulcerations over the gluteal region  Figure 3. Clinical photograph showing pustules and nodules on face 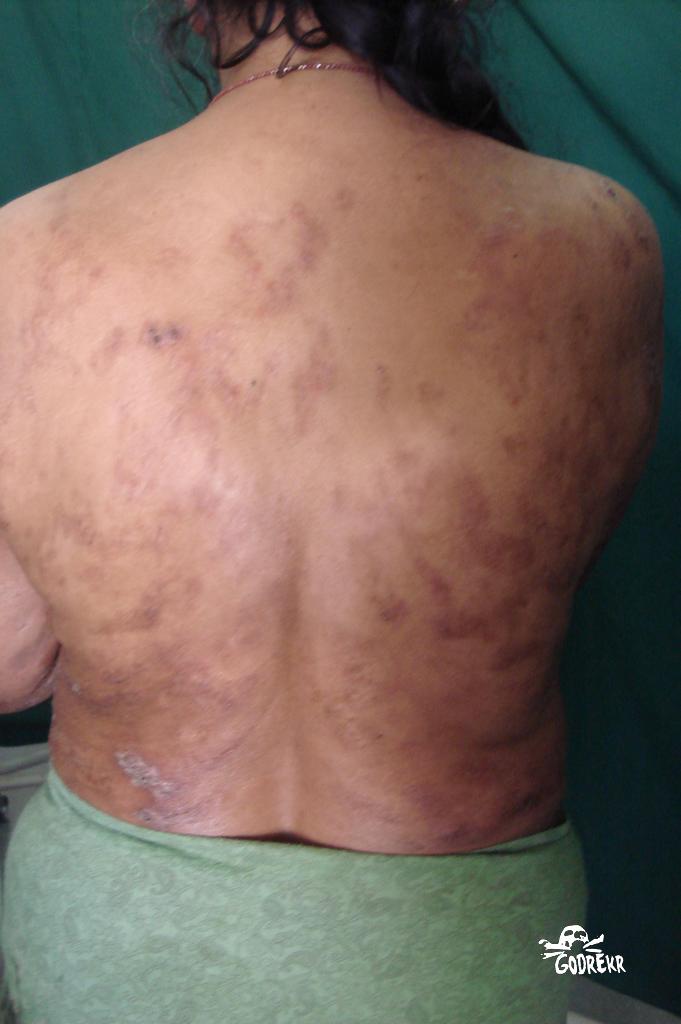 Figure 4. Clinical photograph showing scars an hyperpigmentation A 45 year old lady presented with multiple painful necrotic ulcerations over the trunk, arms, thighs and gluteal areas of two months duration. She also had erythematous papules and pustules over the face since 1 week. History of recurrent papular lesions, some of them undergoing ulceration were present since 3 years. All biochemical parameters were within normal limits. Rheumatoid factor, ANA, Elisa for HIV and VDRL were negative. Pus culture showed growth of Staphylococcus aureus. Smear for AFB showed multiple globi. Skin biopsy showed atrophic epidermis with grenz zone; dermis showed sheets of foamy macrophages and oedematous blood vessels infiltrated with neutrophils and ocasional plasma cells. Patient was admitted and was started on MDT-MB along with thalidomide and prednisolone. -----------------------------------------------------  Figure 1: (a) Hemorrhagic blisters and purpuric macules over dorsum of both the feet (b) Clear fluid filled vesicles and hemorrhagic crusting present along the rim of the right ear  Figure 2: Healing ulcers two and a half months after starting therapy A 38-year-old male, a cook by occupation, was referred to the dermatology clinic from otolaryngology department with blistering over both the hands and feet of 2 days duration. He had been admitted 1 week back with epistaxis and nasopharyngeal myiasis in otolaryngology department. He was started on systemic antibiotics gentamycin, crystalline penicillin, and metronidazole with nasal instillation of turpentine oil 2 drops 6 times a day. Two days later, he had developed edema with painless hemorrhagic blistering over the dorsum of left hand followed by involvement of the right hand, dorsa of both feet, and both the earlobes within a day. Histopathology of the blister showed sub-epidermal blister, with necrotizing leukocytoclastic vasculitis of papillary dermal vessels with thrombosis, numerous acid-fast bacilli in macrophages, and macrophage granulomas extending up to subcutis. In view of the absent fever or constitutional symptoms, and the classical angular infarcts and hemorrhagic blisters evolving into ulcers with angulated margins, we considered LP as the most likely diagnosis. The patient was started on a combination of WHO recommended multibacillary anti-leprosy therapy and prednisolone (40 mg/day).  · |
|
#3
●
07-14-2014, 03:37 AM
| ||||||||
| ***** Cat Poster Rank:283 Female Join Date: Sep 2013 Posts: 4,579
Contributions: 4
Mentioned: 35 Post(s) Quoted: 2595 Post(s)
| ||||||||
|
Re: Lucio's Phenomenon in Leprosy
This is awesome. I'm going to search to see if I can learn more about leprosy here on DR. |
|
#4
●
07-14-2014, 05:08 AM
| ||||||||
| ★ Legacy Member ★ Poster Rank:192 All woman Join Date: Jun 2012 Posts: 7,782 Mentioned: 22 Post(s) Quoted: 1420 Post(s)
| ||||||||
|
Re: Lucio's Phenomenon in Leprosy
Google Carville, Louisiana. It's a town in my home state that was once the site of a flourishing leper colony.
|
|
#8
●
07-15-2014, 02:28 AM
| ||||||||
| ★ Legacy Member ★ Poster Rank:184 female Join Date: Oct 2013 Posts: 8,138 Mentioned: 19 Post(s) Quoted: 1185 Post(s)
| ||||||||
|
Re: Lucio's Phenomenon in Leprosy
What a horrible disease, I had no idea it was still this prevalent, ugh. Poor people. Excellent post, thank you |
























 lothe the leper!” – Rod Flanders
lothe the leper!” – Rod Flanders 




{kind=link}